

Intensity Modulated Proton Therapy for Bilateral Breast or Chest Wall and Comprehensive Nodal Irradiation for Synchronous Bilateral Breast Cancer: Initial Clinical Experience and Dosimetric Comparison
- PMID: 35647397
- PMCID: PMC9133394
- DOI: 10.1016/j.adro.2022.100901
Intensity Modulated Proton Therapy for Bilateral Breast or Chest Wall and Comprehensive Nodal Irradiation for Synchronous Bilateral Breast Cancer: Initial Clinical Experience and Dosimetric Comparison
Abstract
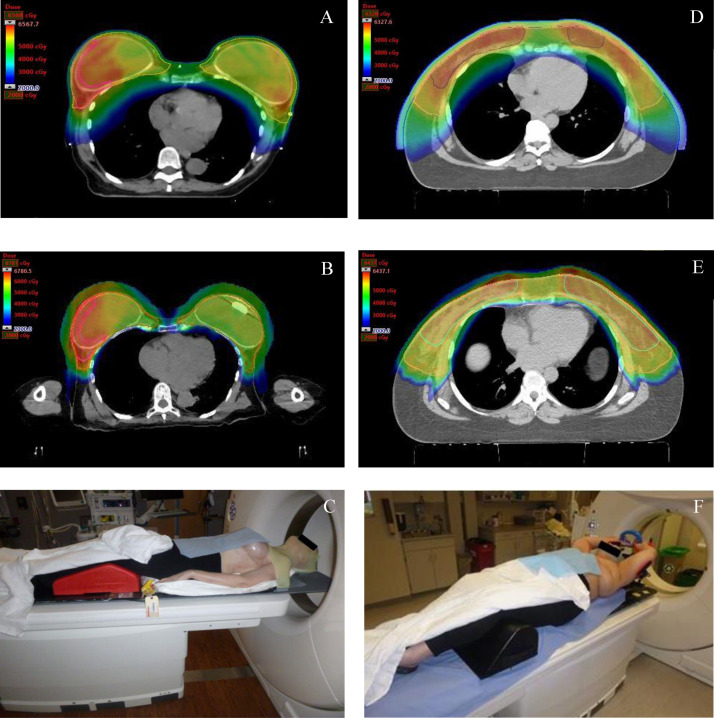
Purpose: Synchronous bilateral breast cancer (SBBC) poses distinct challenges for radiation therapy planning. We report our proton therapy experience in treating patients with SBBC. We also provide a dosimetric comparison of intensity modulated proton therapy (IMPT) versus photon therapy.
Methods and materials: Patients with SBBC who received IMPT at our institution were retrospectively analyzed. The clinical target volume (CTV) included the breast or chest wall and comprehensive regional lymph nodes, including axilla, supraclavicular fossa, and the internal mammary chain. Intensity modulated proton therapy and volumetric modulated arc therapy (VMAT) plans were generated with the goal that 90% of the CTV would recieve at least 90% of the prescription dose (D90>=90%). Comparisons between modalities were made using the Wilcoxon signed rank test. Physician-reported acute toxic effects and photography were collected at baseline, end of treatment, and each follow-up visit.
Results: Between 2015 and 2018, 11 patients with SBBC were treated with IMPT. The prescription was 50 Gy in 25 fractions. The median CTV D90 was 99.9% for IMPT and 97.6% for VMAT (P = .001). The mean heart dose was 0.7 Gy versus 7.2 Gy (P = .001), the total lung mean dose was 7.8 Gy versus 17.3 Gy (P = .001), and the total lung volume recieving 20 Gy was 13.0% versus 27.4% (P = .001). The most common acute toxic effects were dermatitis (mostly grade 1-2 with 1 case of grade 3) and grade 1 to 2 fatigue. The most common toxic effects at the last-follow up (median, 32 months) were grade 1 skin hyperpigmentation, superficial fibrosis, and extremity lymphedema. No nondermatologic or nonfatigue adverse events of grade >1 were recorded.
Conclusions: Bilateral breast and/or chest wall and comprehensive nodal IMPT is technically feasible and associated with low rates of severe acute toxic effects. Treatment with IMPT offered improved target coverage and normal-tissue sparing compared with photon therapy. Long-term follow-up is ongoing to assess efficacy and toxic effects.
© 2022 The Authors.
Figures


References
-
- Heron DE, Komarnicky LT, Hyslop T, Schwartz GF, Mansfield CM. Bilateral breast carcinoma: Risk factors and outcomes for patients with synchronous and metachronous disease. Cancer. 2000;88:2739–2750. - PubMed
-
- Kheirelseid EA, Jumustafa H, Miller N, et al. Bilateral breast cancer: Analysis of incidence, outcome, survival and disease characteristics. Breast Cancer Res Treat. 2011;126:131–140. - PubMed
-
- Gogas J, Markopoulos C, Skandalakis P, Gogas H. Bilateral breast cancer. Am Surg. 1993;59:733–735. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
