

Do new trauma centers provide needed or redundant access? A nationwide analysis
- PMID: 35647793
- PMCID: PMC9615221
- DOI: 10.1097/TA.0000000000003652
Do new trauma centers provide needed or redundant access? A nationwide analysis
Abstract
Background: Our prior research has demonstrated that increasing the number of trauma centers (TCs) in a state does not reliably improve state-level injury-related mortality. We hypothesized that many new TCs would serve populations already served by existing TCs, rather than in areas without ready TC access. We also hypothesized that new TCs would also be less likely to serve economically disadvantaged populations.
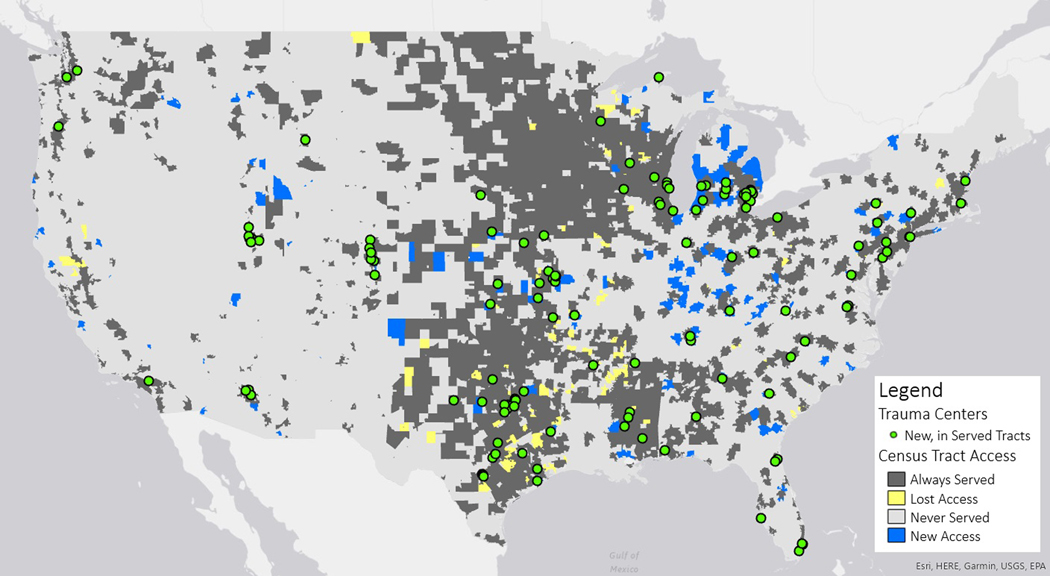
Methods: All state-designated adult TCs registered with the American Trauma Society in 2014 and 2019 were mapped using ArcGIS Pro (ESRI Inc., Redlands, CA). Trauma centers were grouped as Level 1 or 2 (Lev12) or Level 3, 4 or 5 (Lev345). We also obtained census tract-level data (73,666 tracts), including population counts and percentage of population below the federal poverty threshold. Thirty-minute drive-time areas were created around each TC. Census tracts were considered "served" if their geographic centers were located within a 30-minute drive-time area to any TC. Data were analyzed at the census tract level.
Results: A total of 2,140 TCs were identified in 2019, with 256 new TCs and 151 TC closures. Eighty-two percent of new TCs were Levels 3 to 5. Nationwide, coverage increased from 75.3% of tracts served in 2014 to 78.1% in 2019, representing an increased coverage from 76.0% to 79.4% of the population. New TC served 17,532 tracts, of which 87.3% were already served. New Lev12 TCs served 9,100 tracts, of which 91.2% were already served; new Lev345 TCs served 15,728 tracts, of which 85.9% were already served. Of 2,204 newly served tracts, those served by Lev345 TCs had higher mean percentage poverty compared with those served by Lev12 TCs (15.7% vs. 13.2% poverty, p < 0.05).
Discussion: Overall, access to trauma care has been improving in the United States. However, the majority of new TCs opened in locations with preexisting access to trauma care. Nationwide, Levels 3, 4, and 5 TCs have been responsible for expanding access to underserved populations.
Level of evidence: Prognostic and Epidemiologic; Level IV.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest:
Dr. Ho spouse is a consultant for Medtronic, Zimmer Biomet, Atricure, and Astra Zeneca.
Drs. Ferre, Curtis, Flippin, Claridge, Tseng, and Brown have no financial ties to disclose.
Figures
References
-
- Dodson BK, Braswell M, David AP, Young JS, Riccio LM, Kim Y, et al. Adult and elderly population access to trauma centers: an ecological analysis evaluating the relationship between injury-related mortality and geographic proximity in the United States in 2010. J Public Health (Oxf). 2018;40(4):848–57. - PMC - PubMed
-
- Mann NC, Mullins RJ, MacKenzie EJ, Jurkovich GJ, Mock CN. Systematic review of published evidence regarding trauma system effectiveness. J Trauma. 1999;47(3 Suppl):S25–33. - PubMed
-
- Nathens AB, Jurkovich GJ, Rivara FP, Maier RV. Effectiveness of state trauma systems in reducing injury-related mortality: a national evaluation. J Trauma. 2000;48(1):25–30; discussion −1. - PubMed
-
- Nathens AB, Jurkovich GJ, Cummings P, Rivara FP, Maier RV. The effect of organized systems of trauma care on motor vehicle crash mortality. JAMA. 2000;283(15):1990–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
