

Sympathetic ophthalmia: A comprehensive update
- PMID: 35647958
- PMCID: PMC9359263
- DOI: 10.4103/ijo.IJO_2363_21
Sympathetic ophthalmia: A comprehensive update
Abstract
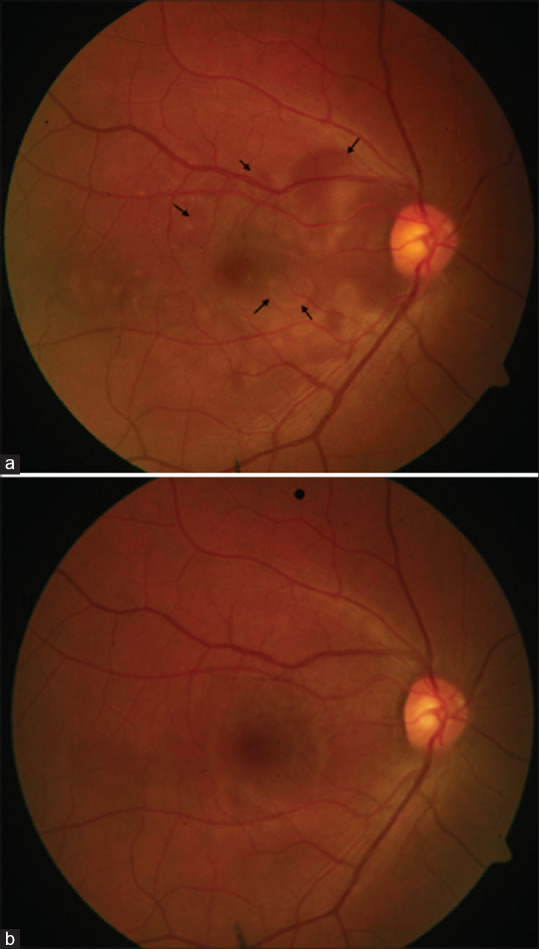
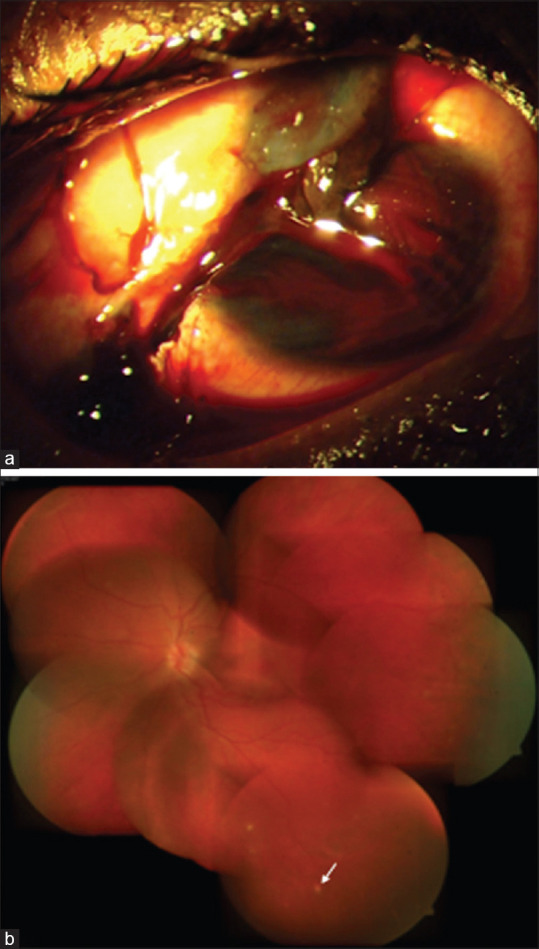
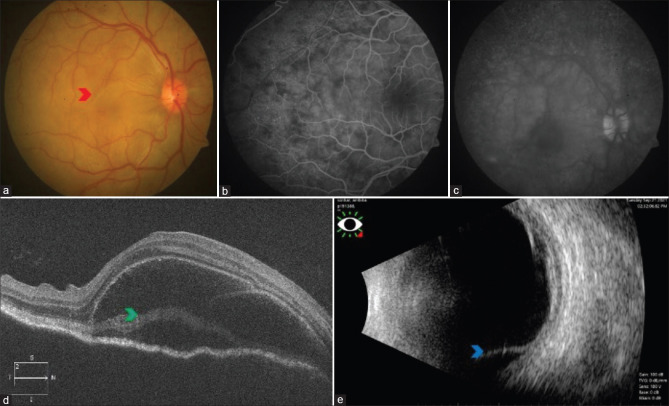
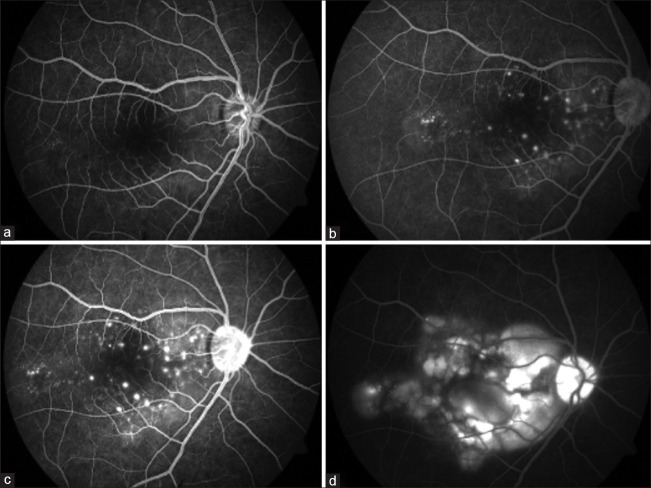
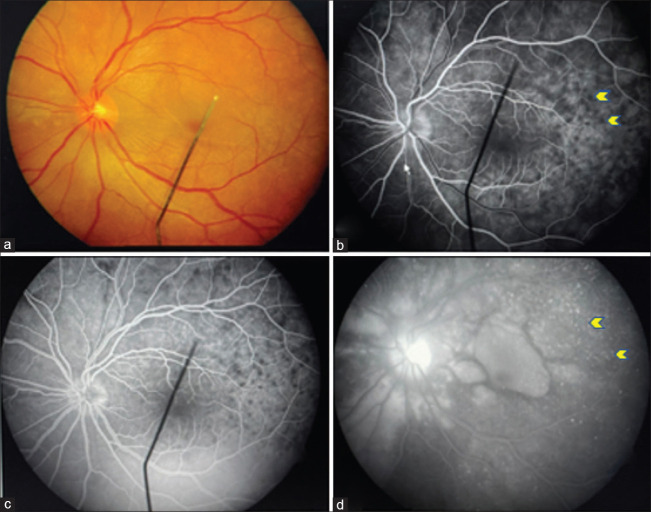
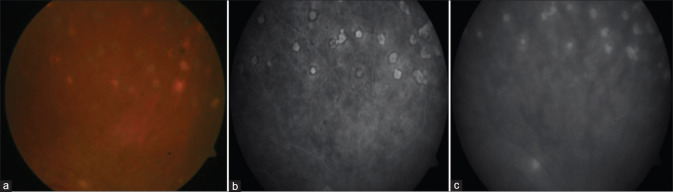
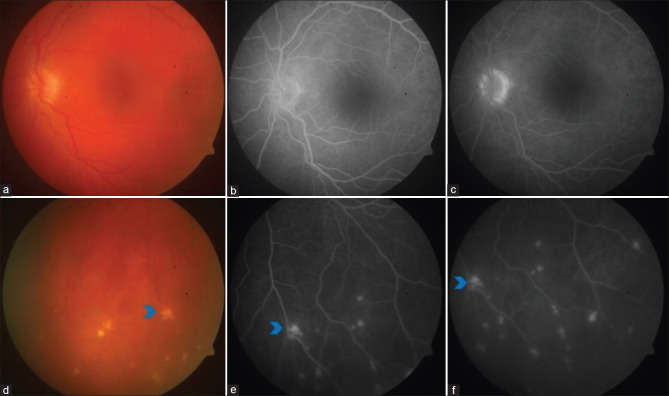
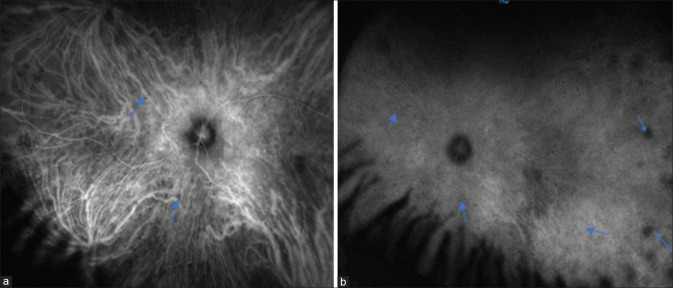
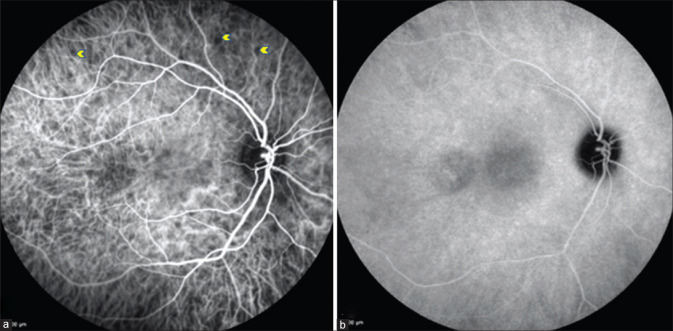
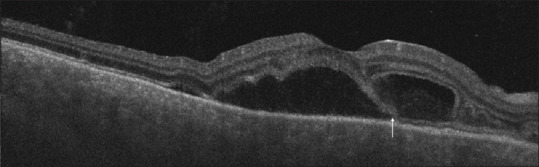
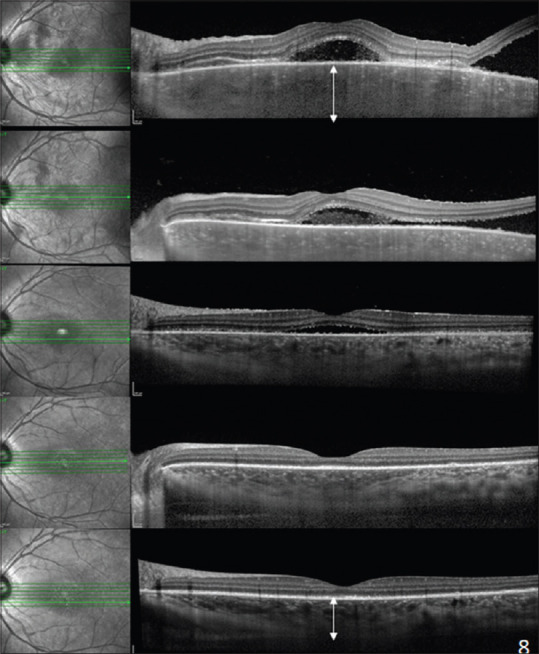
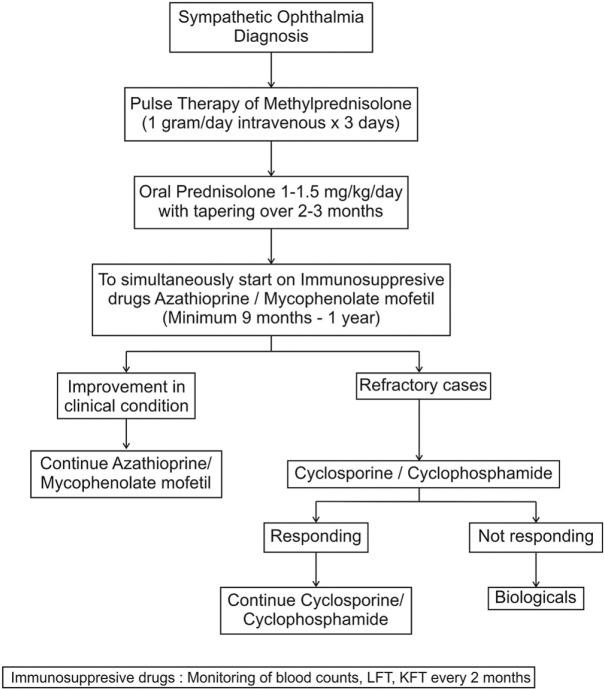
Sympathetic ophthalmia is a rare, bilateral, granulomatous, panuveitis following penetrating trauma or surgery to one eye. Clinical presentation commonly occurs within the first year of trauma occurrence but can be delayed by several years. It manifests as acute/chronic granulomatous uveitis with yellowish-white choroidal lesions or Dalen-Fuchs nodules. Initially, patients respond rapidly to corticosteroid therapy, but a majority require long-term use of corticosteroid-sparing agents to prevent recurrences. The purpose of this review is to elaborate on the current understanding of the pathophysiology, the importance of multimodal imaging in early diagnosis, and the role of newer immunomodulatory and biological agents in recalcitrant cases.
Keywords: Dalen–Fuchs nodule; granulomatous uveitis; immunosuppression; ocular trauma; panuveitis; sympathetic ophthalmia.
Conflict of interest statement
None
Figures

References
-
- Albert D, Diaz-Rohena R. A historical review of sympathetic ophthalmia and its epidemiology. Surv Ophthalmol. 1989;34:1–14. - PubMed
-
- Mackenzie W. 3rd edition. London: Longmans; 1840. A Practical Treatise on the Diseases of the Eye; pp. 523–34.
-
- Dalen A. Zur Kenntnis der sogenannten Choroiditis sympathetica. Mitt Augen Klin Carolin Med. Chirurg Inst Stockholm. 1904;6:1.
-
- Fuchs E. On sympathetic inflammation (initially remarks on serous iritis) Graefes Arch Clinical Exp Ophthalmology. 1905;61:365–456.
-
- Elschnig A. Studies on sympathetic ophthalmia, II:The antigenic effects of eye pigments. Graefes Arch Clin Exp Ophthalmol. 1910;76:509–46.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
