

Magnetic resonance imaging of inflammatory pseudotumor of the liver: a 2021 systematic literature update and series presentation
- PMID: 35648207
- PMCID: PMC9300573
- DOI: 10.1007/s00261-022-03555-9
Magnetic resonance imaging of inflammatory pseudotumor of the liver: a 2021 systematic literature update and series presentation
Abstract
Purpose: Inflammatory pseudotumors of the liver (IPTL) are not exceptional benign lesions with various etiologies, histology, and imaging appearances. The incomplete knowledge of this pathology and the wide polymorphism sometimes resembling malignancy often induce long and expensive diagnostic flow, biopsy and occasionally unnecessary surgery. We propose a systematic revision of MRI literature data (2000-2021) with some narrative inserts and 10 new complete MRI cases, with the aim of organizing the data about IPTL and identifying some typical features able to improve its diagnosis from imaging.
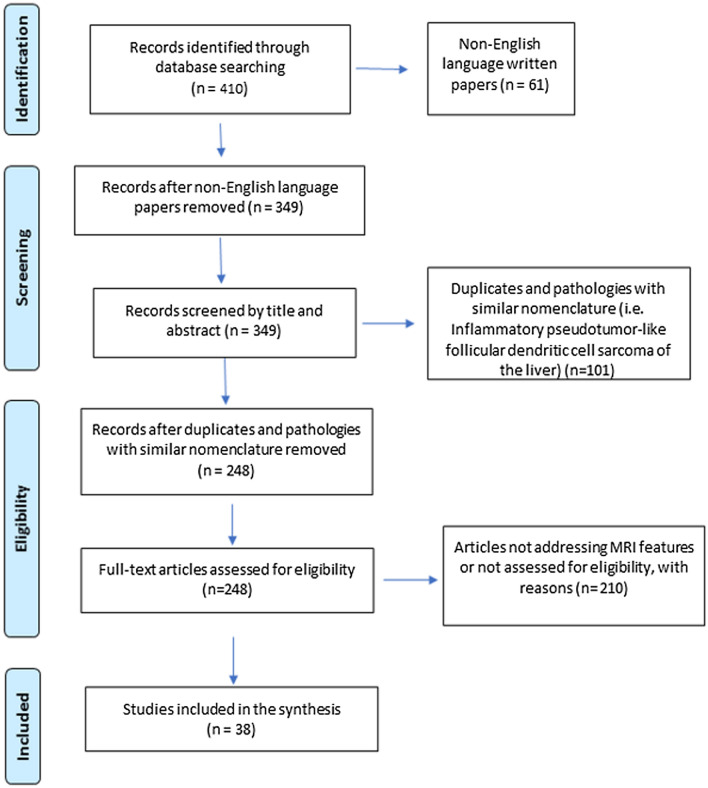
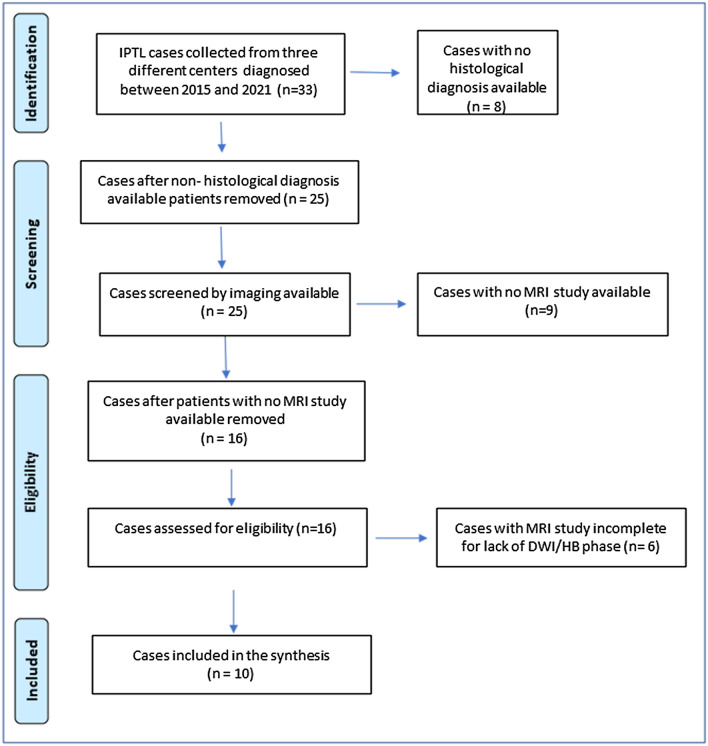
Methods: We performed a systematic revision of literature from 2000 to 2021 to obtain MRI features, epidemiological, and clinical data of IPTL. The basic online search algorithm on the PubMed database was "(pseudotumor) AND (liver) AND (imaging)." Quality assessment was performed using both scales by Moola for case report studies and by Munn for cross-sectional studies reporting prevalence data. A case-based retrospective study by collecting patients diagnosed with IPTL from three different university hospitals from 2015 to 2021 was done as well. Only cases with MR examinations complete with T1/T2/contrast-enhanced T1/Diffusion-Weighted (W) images and pathology-proven IPTL were selected.
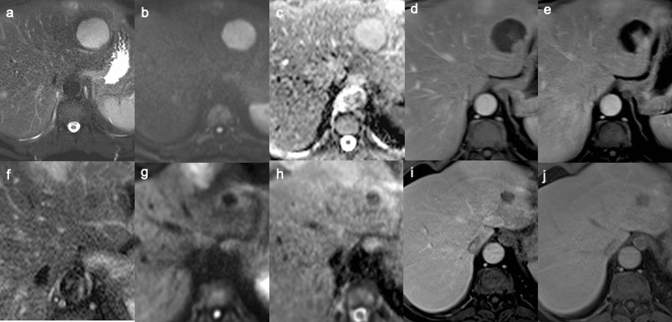
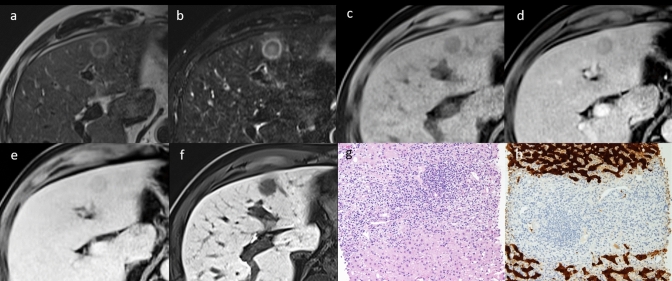
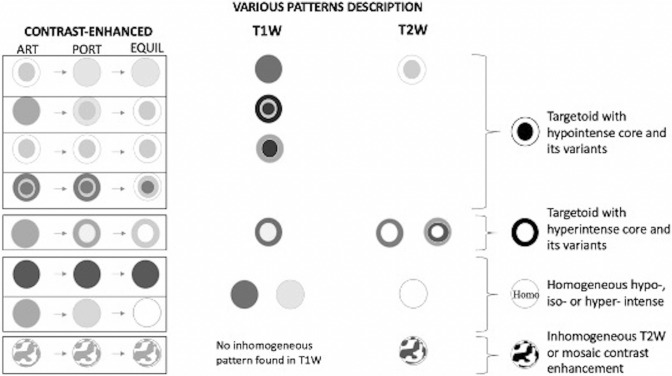
Results: After screening/selection 38 articles were included for a total of 114 patients. In our experience we selected 10 cases for a total of 16 IPTLs; 8 out of 10 patients underwent at least 1 MRI follow-up. Some reproducible and rather typical imaging findings for IPTL were found. The targetoid aspect of IPTL is very frequent in our experience (75% on T1W, 44% on T2W, 81% on contrast-enhanced T1W (at least one phase), 100% on Diffusion-W images) but is also recurrent in the literature (6% on T1W, 31% on T2W, 51% on CE-T1W (at least one phase), 18% on Diffusion-W images, and 67% on hepatobiliary phase). In our experience, Apparent Diffusion Coefficient map values were always equal to or higher than those of the surrounding parenchyma, and at MRI follow-up, nodule/s disappeared at first/second control, in six patients, while in the remaining 2, lesions persisted with tendency to dehydration.
Conclusion: A targetoid-like aspect of a focal liver lesion must raise diagnostic suspicion, especially if IgG4-positive plasma is detected. MRI follow-up mainly shows the disappearance of the lesion or its reduction with dehydration.
Keywords: Focal liver lesion; IgG4-related disease; Inflammatory pseudotumor of the liver; Magnetic resonance imaging; Targetoid aspect.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that there are no conflicts of interest regarding the publication of this article.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
