

Contrast-enhanced mammography for the assessment of screening recalls: a two-centre study
- PMID: 35648209
- PMCID: PMC9668944
- DOI: 10.1007/s00330-022-08868-3
Contrast-enhanced mammography for the assessment of screening recalls: a two-centre study
Abstract
Objectives: To evaluate the potential of contrast-enhanced mammography (CEM) for reducing the biopsy rate of screening recalls.
Methods: Recalled women were prospectively enrolled to undergo CEM alongside standard assessment (SA) through additional views, tomosynthesis, and/or ultrasound. Exclusion criteria were symptoms, implants, allergy to contrast agents, renal failure, and pregnancy. SA and CEM were independently evaluated by one of six radiologists, who recommended biopsy or 2-year follow-up. Biopsy rates according to SA or recombined CEM (rCEM) were compared with the McNemar's test. Diagnostic performance was calculated considering lesions with available final histopathology.
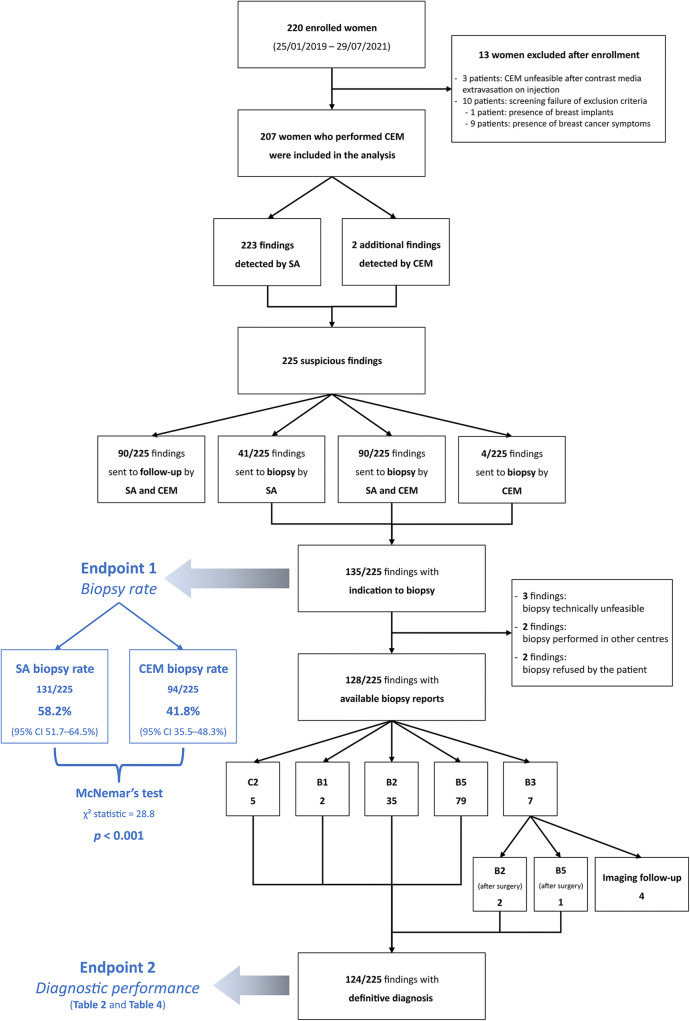
Results: Between January 2019 and July 2021, 220 women were enrolled, 207 of them (median age 56.6 years) with 225 suspicious findings analysed. Three of 207 patients (1.4%) developed mild self-limiting adverse reactions to iodinated contrast agent. Overall, 135/225 findings were referred for biopsy, 90/225 by both SA and rCEM, 41/225 by SA alone and 4/225 by rCEM alone (2/4 being one DCIS and one invasive carcinoma). The rCEM biopsy rate (94/225, 41.8%, 95% CI 35.5-48.3%) was 16.4% lower (p < 0.001) than the SA biopsy rate (131/225, 58.2%, 95% CI 51.7-64.5%). Considering the 124/135 biopsies with final histopathology (44 benign, 80 malignant), rCEM showed a 93.8% sensitivity (95% CI 86.2-97.3%) and a 65.9% specificity (95% CI 51.1-78.1%), all 5 false negatives being ductal carcinoma in situ detectable as suspicious calcifications on low-energy images.
Conclusions: Compared to SA, the rCEM-based work-up would have avoided biopsy for 37/225 (16.4%) suspicious findings. Including low-energy images in interpretation provided optimal overall CEM sensitivity.
Key points: • The work-up of suspicious findings detected at mammographic breast cancer screening still leads to a high rate of unnecessary biopsies, involving between 2 and 6% of screened women. • In 207 recalled women with 225 suspicious findings, recombined images of contrast-enhanced mammography (CEM) showed a 93.8% sensitivity and a 65.9% specificity, all 5 false negatives being ductal carcinoma in situ detectable on low-energy images as suspicious calcifications. • CEM could represent an easily available one-stop shop option for the morphofunctional assessment of screening recalls, potentially reducing the biopsy rate by 16.4%.
Keywords: Biopsy, needle; Breast neoplasms; Ductal carcinoma in situ; Mammography, contrast-enhanced; Mass screening.
© 2022. The Author(s).
Conflict of interest statement
Andrea Cozzi, Marianna Fanizza, and Veronica Magni controlled and analysed the data. None of them has relationships with any companies, whose products or services may be related to the subject matter of the article.
Simone Schiaffino received travel support from Bracco Imaging and is a member of the speakers’ bureau for GE Healthcare.
Francesco Sardanelli received research grants from — and is a member of the speakers’ bureau of — GE Healthcare, Bayer, and Bracco; he is also a member of the Bracco Advisory Group.
All other authors declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures

Comment in
-
Contrast-enhanced mammography for screening recalls: a problem-solving assessment tool ready for use?Eur Radiol. 2022 Nov;32(11):7386-7387. doi: 10.1007/s00330-022-09094-7. Epub 2022 Sep 13. Eur Radiol. 2022. PMID: 36100775 No abstract available.
