

cDC1 Vaccines Drive Tumor Rejection by Direct Presentation Independently of Host cDC1
- PMID: 35648641
- PMCID: PMC9357132
- DOI: 10.1158/2326-6066.CIR-21-0865
cDC1 Vaccines Drive Tumor Rejection by Direct Presentation Independently of Host cDC1
Abstract
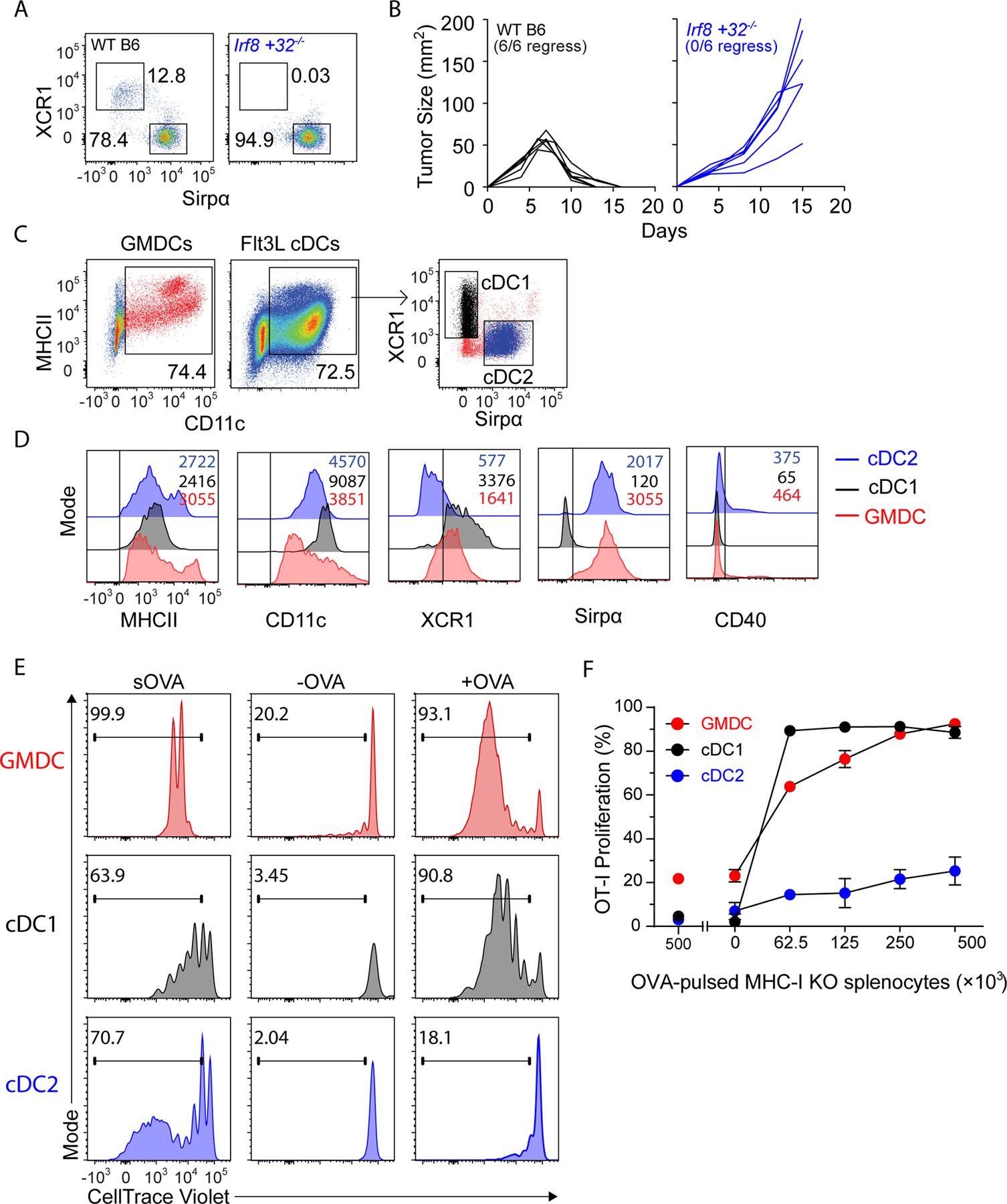
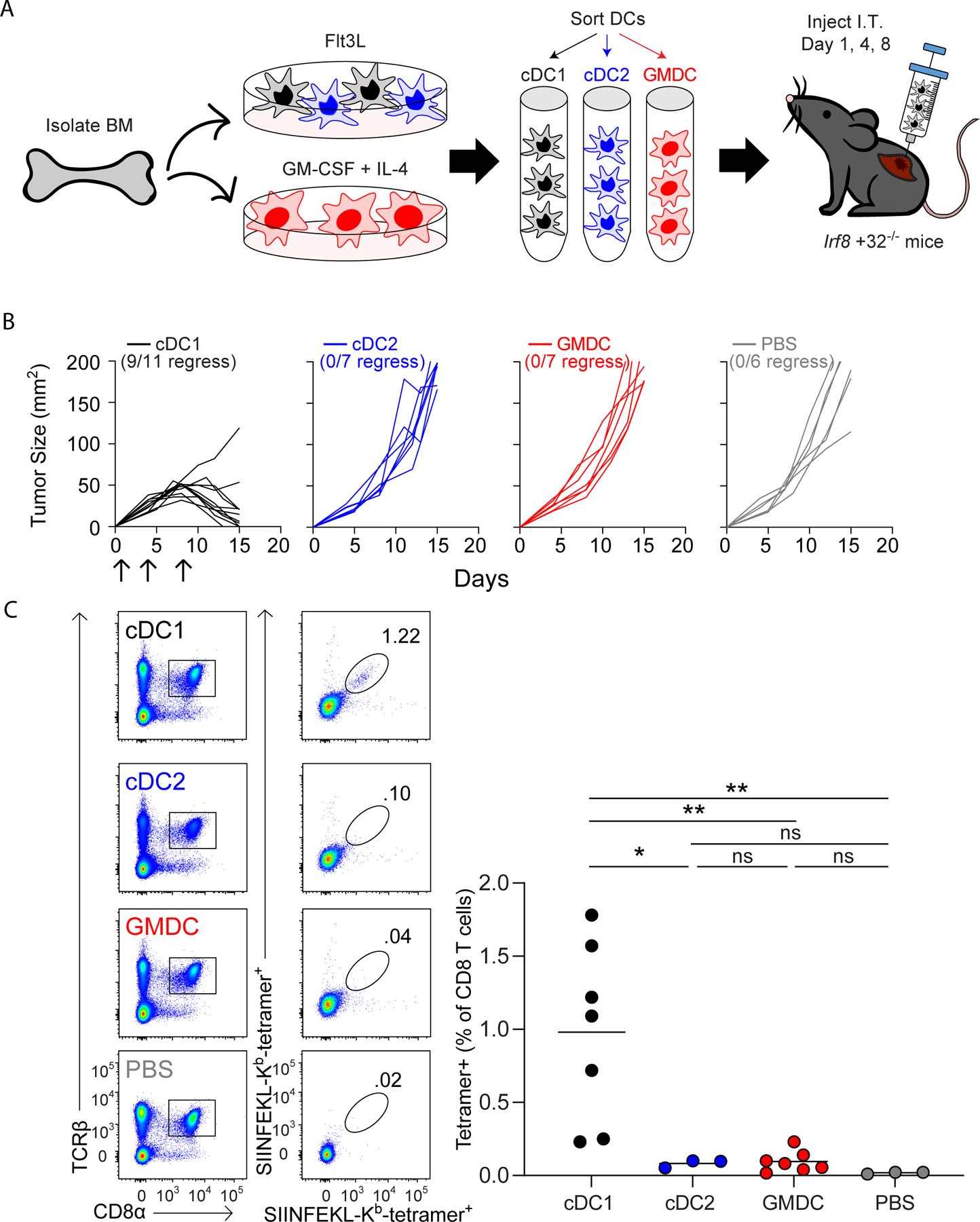
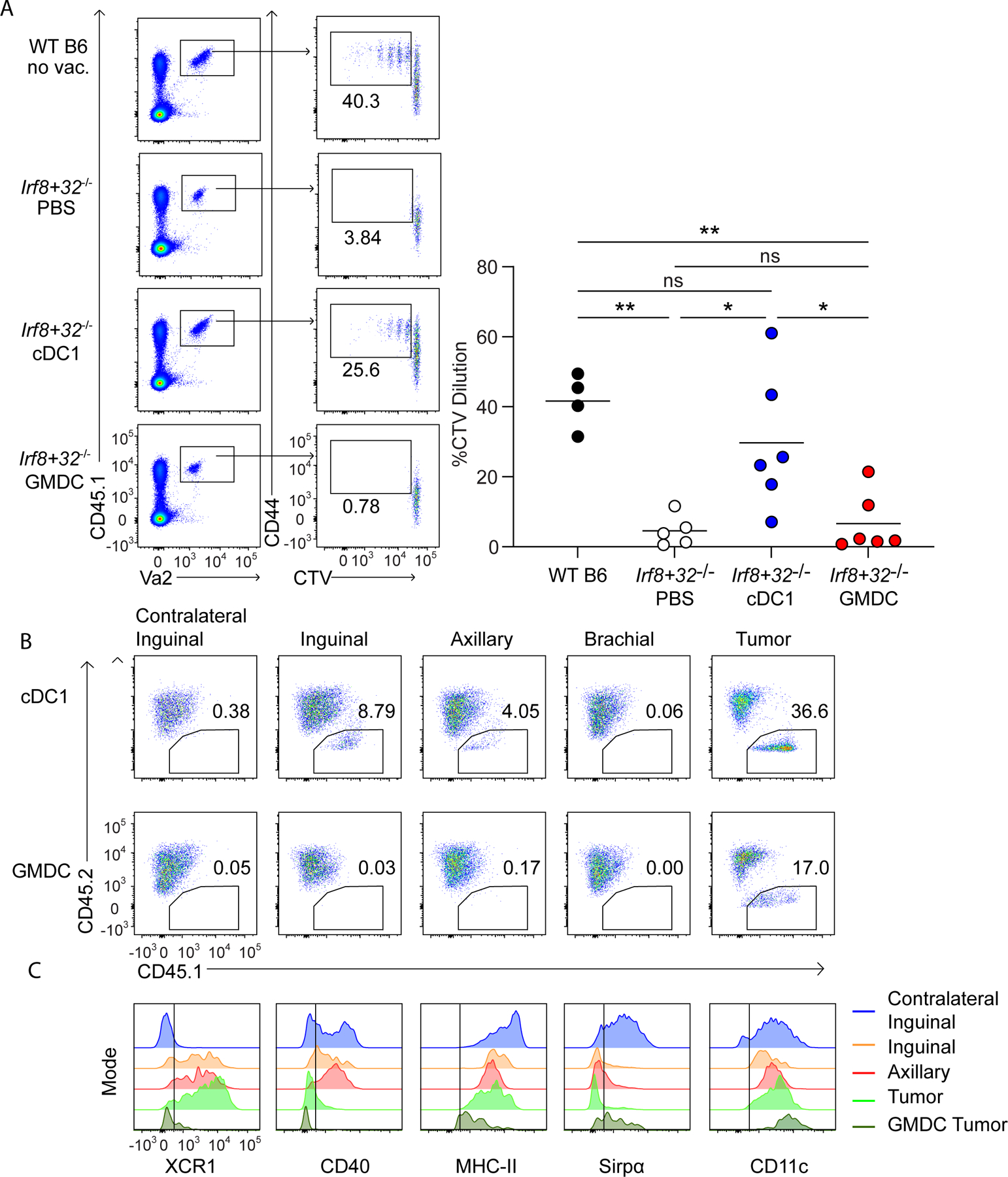
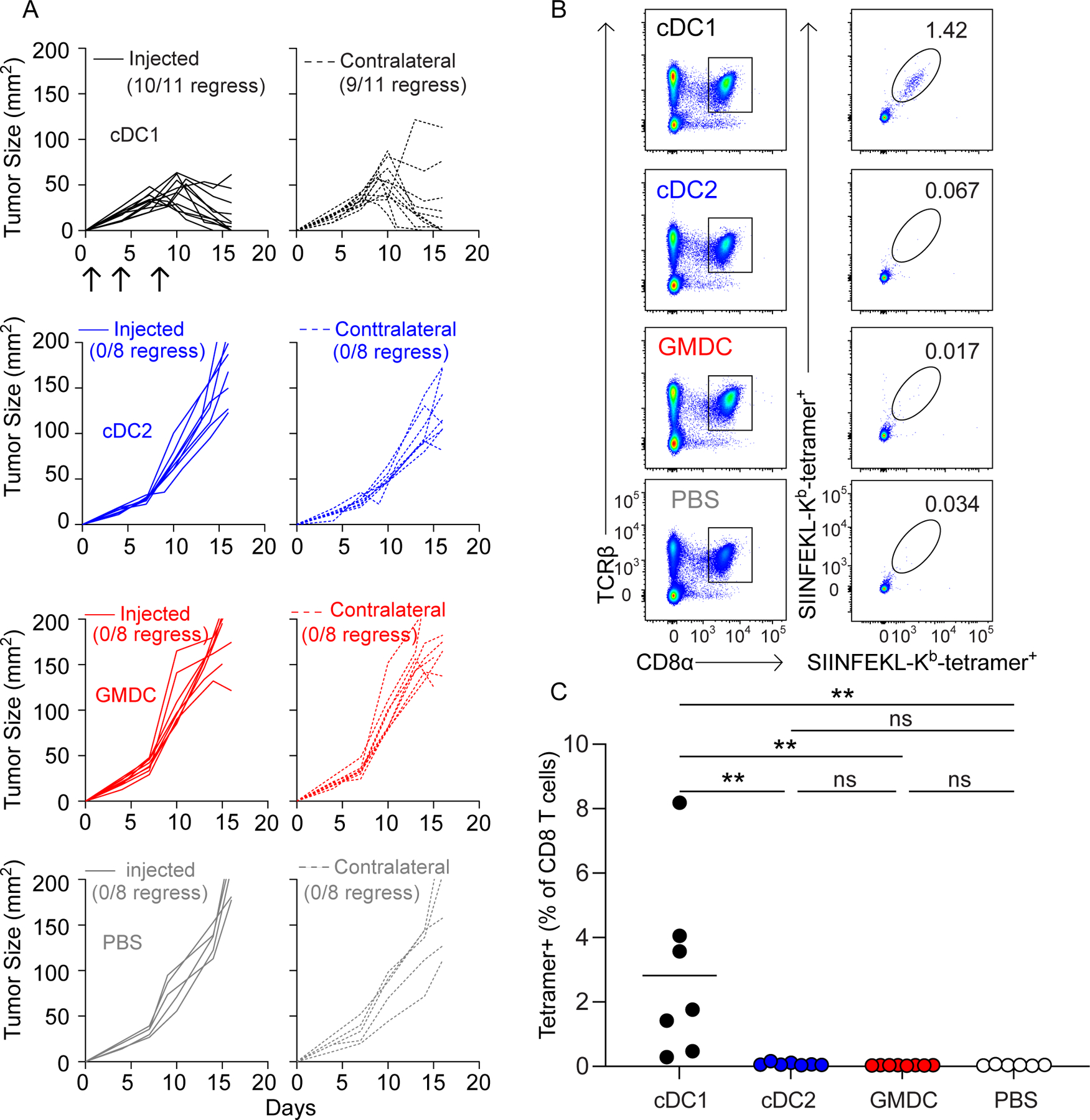
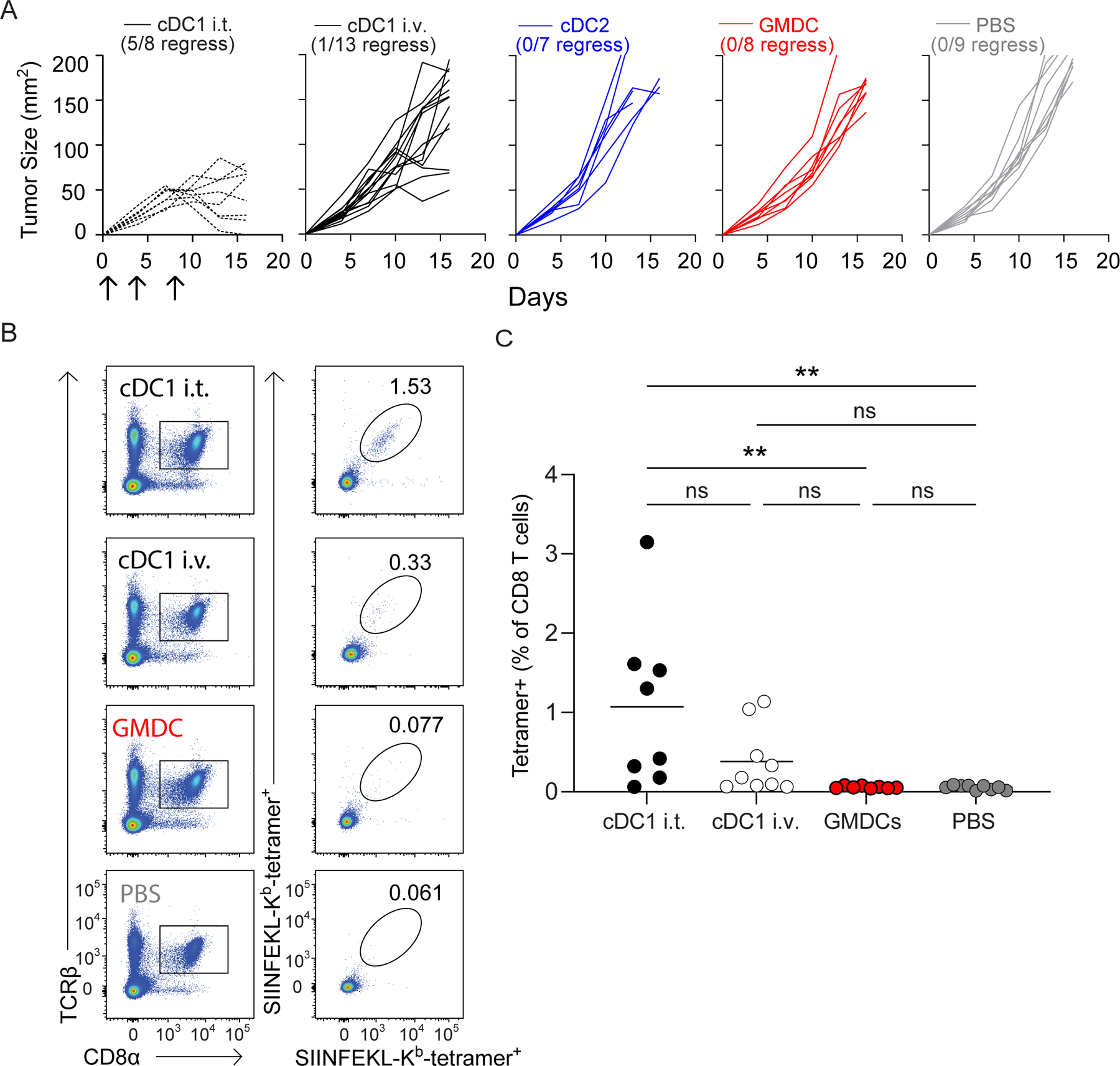
As a cell-based cancer vaccine, dendritic cells (DC), derived from peripheral blood monocytes or bone marrow (BM) treated with GM-CSF (GMDC), were initially thought to induce antitumor immunity by presenting tumor antigens directly to host T cells. Subsequent work revealed that GMDCs do not directly prime tumor-specific T cells, but must transfer their antigens to host DCs. This reduces their advantage over strictly antigen-based strategies proposed as cancer vaccines. Type 1 conventional DCs (cDC1) have been reported to be superior to GMDCs as a cancer vaccine, but whether they act by transferring antigens to host DCs is unknown. To test this, we compared antitumor responses induced by GMDCs and cDC1 in Irf8 +32-/- mice, which lack endogenous cDC1 and cannot reject immunogenic fibrosarcomas. Both GMDCs and cDC1 could cross-present cell-associated antigens to CD8+ T cells in vitro. However, injection of GMDCs into tumors in Irf8 +32-/- mice did not induce antitumor immunity, consistent with their reported dependence on host cDC1. In contrast, injection of cDC1s into tumors in Irf8 +32-/- mice resulted in their migration to tumor-draining lymph nodes, activation of tumor-specific CD8+ T cells, and rejection of the tumors. Tumor rejection did not require the in vitro loading of cDC1 with antigens, indicating that acquisition of antigens in vivo is sufficient to induce antitumor responses. Finally, cDC1 vaccination showed abscopal effects, with rejection of untreated tumors growing concurrently on the opposite flank. These results suggest that cDC1 may be a useful future avenue to explore for antitumor therapy. See related Spotlight by Hubert et al., p. 918.
©2022 American Association for Cancer Research.
Conflict of interest statement
Figures
Comment in
-
Direct T-cell Presentation by cDC1: The Key Feature for Cancer Vaccine Success?Cancer Immunol Res. 2022 Aug 3;10(8):918. doi: 10.1158/2326-6066.CIR-22-0473. Cancer Immunol Res. 2022. PMID: 35802596
Comment on
-
Direct T-cell Presentation by cDC1: The Key Feature for Cancer Vaccine Success?Cancer Immunol Res. 2022 Aug 3;10(8):918. doi: 10.1158/2326-6066.CIR-22-0473. Cancer Immunol Res. 2022. PMID: 35802596
References
-
- Sims RB. Development of sipuleucel-T: autologous cellular immunotherapy for the treatment of metastatic castrate resistant prostate cancer. Vaccine 2012;30:4394–4397. - PubMed
-
- Helft J, Bottcher J, Chakravarty P, Zelenay S, Huotari J, Schraml BU et al. GM-CSF Mouse Bone Marrow Cultures Comprise a Heterogeneous Population of CD11c(+)MHCII(+) Macrophages and Dendritic Cells. Immunity 2015;42:1197–1211. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
