

Integration of Genomic Biology Into Therapeutic Strategies of Gastric Cancer Peritoneal Metastasis
- PMID: 35649219
- PMCID: PMC9390822
- DOI: 10.1200/JCO.21.02745
Integration of Genomic Biology Into Therapeutic Strategies of Gastric Cancer Peritoneal Metastasis
Abstract
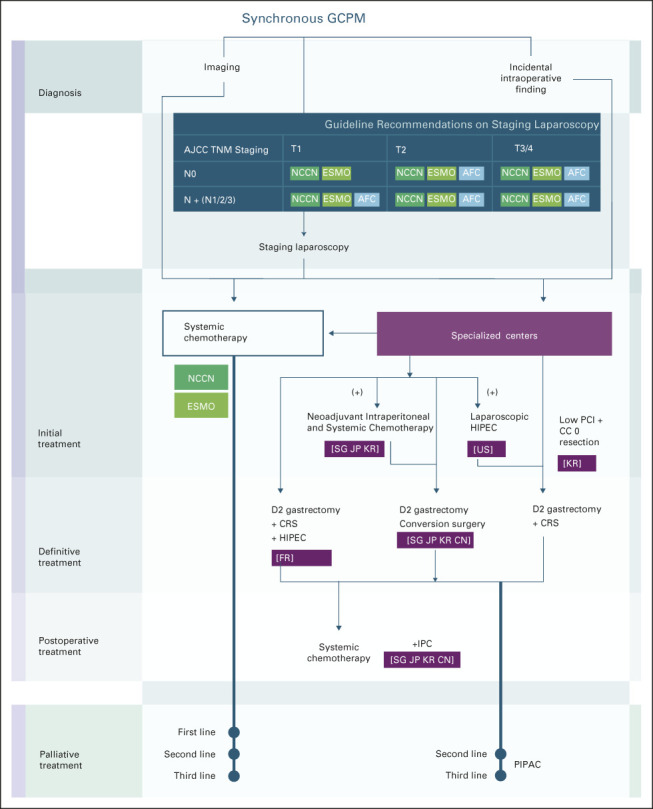
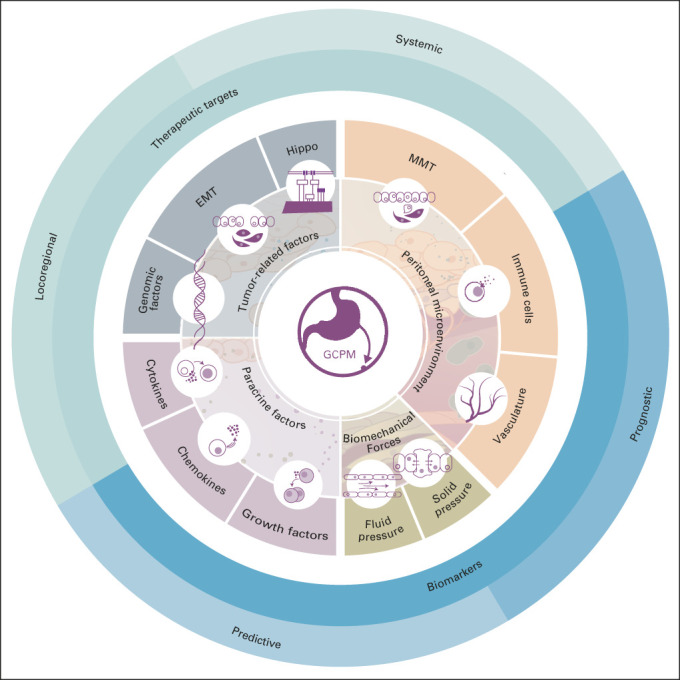
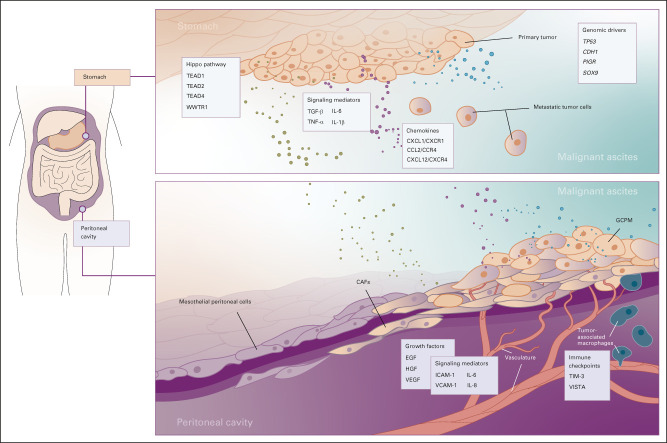
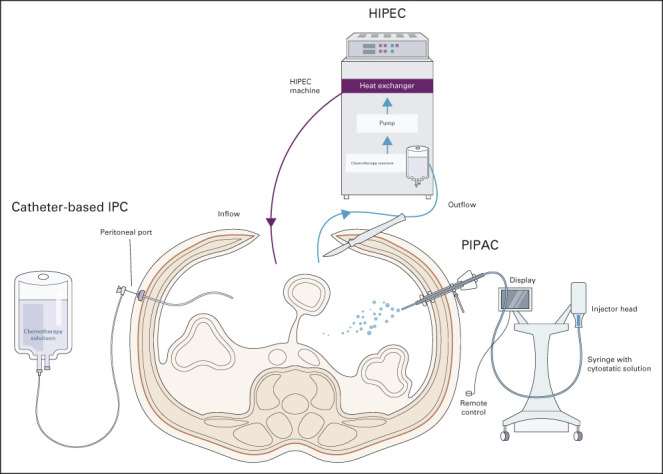
The peritoneum is a common site of metastasis in advanced gastric cancer (GC). Diagnostic laparoscopy is now routinely performed as part of disease staging, leading to an earlier diagnosis of synchronous peritoneal metastasis (PM). The biology of GCPM is unique and aggressive, leading to a dismal prognosis. These tumors tend to be resistant to traditional systemic therapy, and yet, this remains the current standard-of-care recommended by most international clinical guidelines. As this is an area of unmet clinical need, several translational studies and clinical trials have focused on addressing this specific disease state. Advances in genomic sequencing and molecular profiling have revealed several promising therapeutic targets and elucidated novel biology, particularly on the role of the surrounding tumor microenvironment in GCPM. Peritoneal-specific clinical trials are being designed with a combination of locoregional therapeutic strategies with systemic therapy. In this review, we summarize the new knowledge of cancer biology, advances in surgical techniques, and emergence of novel therapies as an integrated strategy emerges to address GCPM as a distinct clinical entity.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, et al. : Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71:209-249, 2021 - PubMed
-
- Koemans WJ, Lurvink RJ, Grootscholten C, et al. : Synchronous peritoneal metastases of gastric cancer origin: Incidence, treatment and survival of a nationwide Dutch cohort. Gastric Cancer 24:800-809, 2021 - PubMed
-
- Eisenhauer EA, Therasse P, Bogaerts J, et al. : New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer 45:228-247, 2009 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
