

Clinicodemographic profile and predictors of poor outcome in hospitalised COVID-19 patients: a single-centre, retrospective cohort study from India
- PMID: 35649611
- PMCID: PMC9160596
- DOI: 10.1136/bmjopen-2021-056464
Clinicodemographic profile and predictors of poor outcome in hospitalised COVID-19 patients: a single-centre, retrospective cohort study from India
Abstract
Objectives: Primary objective was to study the clinicodemographic profile of hospitalised COVID-19 patients at a tertiary-care centre in India. Secondary objective was to identify predictors of poor outcome.
Setting: Single centre tertiary-care level.
Design: Retrospective cohort study.
Participants: Consecutively hospitalised adults patients with COVID-19.
Primary and secondary outcome measures: Primary outcome variable was in-hospital mortality. Covariables were known comorbidities, clinical features, vital signs at the time of admission and on days 3-5 of admission, and initial laboratory investigations.
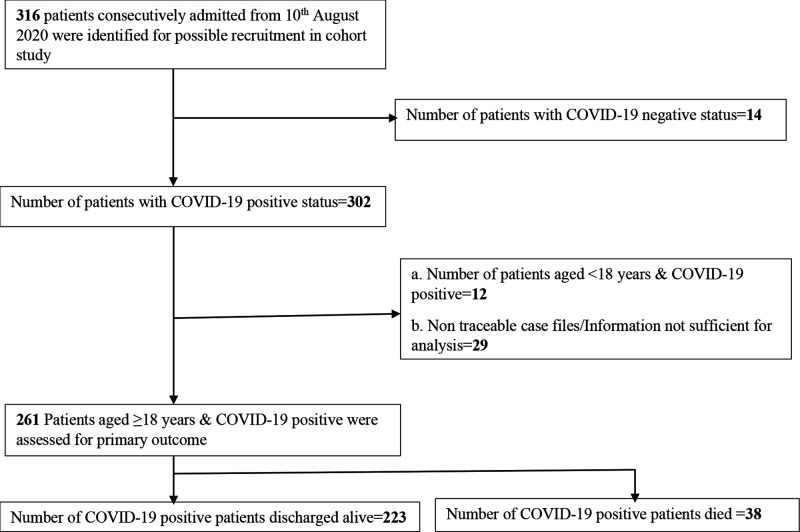
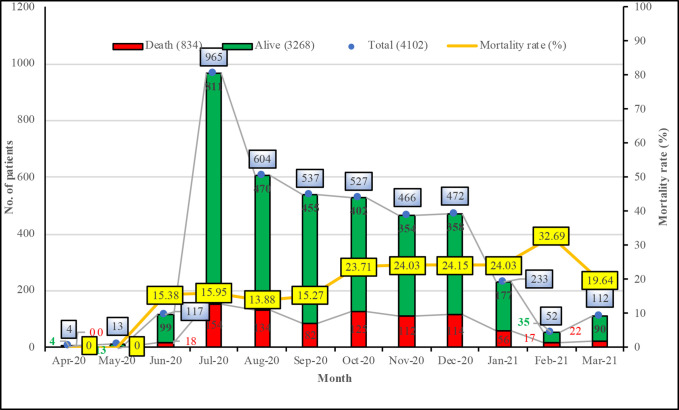
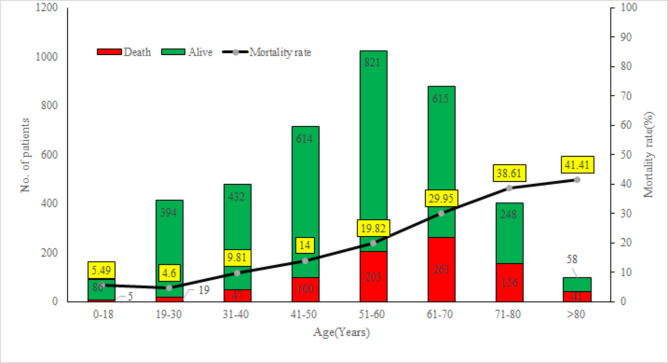
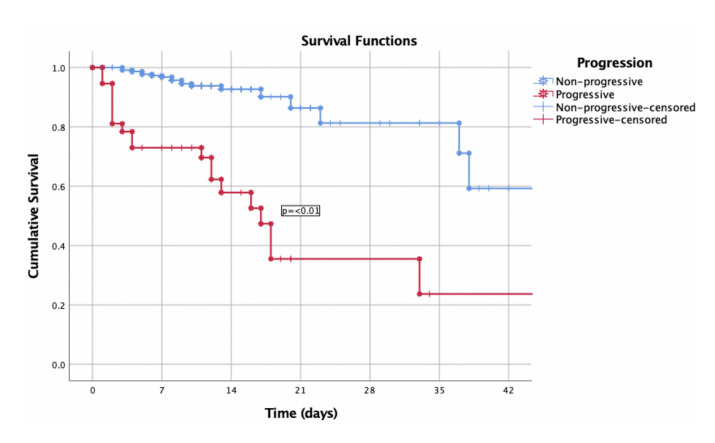
Results: Intergroup differences were tested using χ2 or Fischer's exact tests, Student's t-test or Mann-Whitney U test. Predictors of mortality were evaluated using multivariate logistic regression model. Out of 4102 SARS-CoV-2 positive patients admitted during 1-year period, 3268 (79.66%) survived to discharge and 834 (20.33%) died in the hospital. Mortality rates increased with age. Death was more common among males (OR 1.51, 95% CI 1.25 to 1.81). Out of 261 cases analysed in detail, 55.1% were in mild, 32.5% in moderate and 12.2% in severe triage category. Most common clinical presentations in the subgroup were fever (73.2%), cough/coryza (65.5%) and breathlessness (54%). Hypertension (45.2%), diabetes mellitus (41.8%) and chronic kidney disease (CKD; 6.1%) were common comorbidities. Disease severity on admission (adjusted OR 12.53, 95% CI 4.92 to 31.91, p<0.01), coagulation defect (33.21, 3.85-302.1, p<0.01), CKD (5.67, 1.08-29.64, p=0.04), high urea (11.05, 3.9-31.02, p<0.01), high prothrombin time (3.91, 1.59-9.65, p<0.01) and elevated ferritin (1.02, 1.00-1.03, p=0.02) were associated with poor outcome on multivariate regression. A strong predictor of mortality was disease progression on days 3-5 of admission (adjusted OR 13.66 95% CI 3.47 to 53.68).
Conclusion: COVID-19 related mortality in hospitalised adult patients at our center was similar to the developed countries. Progression in disease severity on days 3-5 of admission or days 6-13 of illness onset acts as 'turning point' for timely referral or treatment intensification for optimum use of resources.
Keywords: covid-19; epidemiology; international health services; public health.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Coronavirus in India: Latest Map and Case Count [Internet]. Available: https://www.covid19india.org [Accessed 15 May 2021].
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous