

Whole genome sequencing reveals hidden transmission of carbapenemase-producing Enterobacterales
- PMID: 35650193
- PMCID: PMC9160272
- DOI: 10.1038/s41467-022-30637-5
Whole genome sequencing reveals hidden transmission of carbapenemase-producing Enterobacterales
Abstract
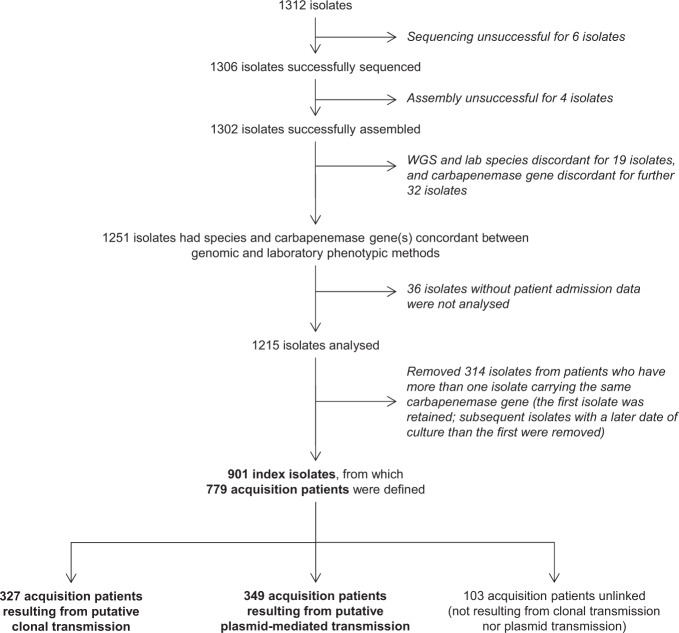
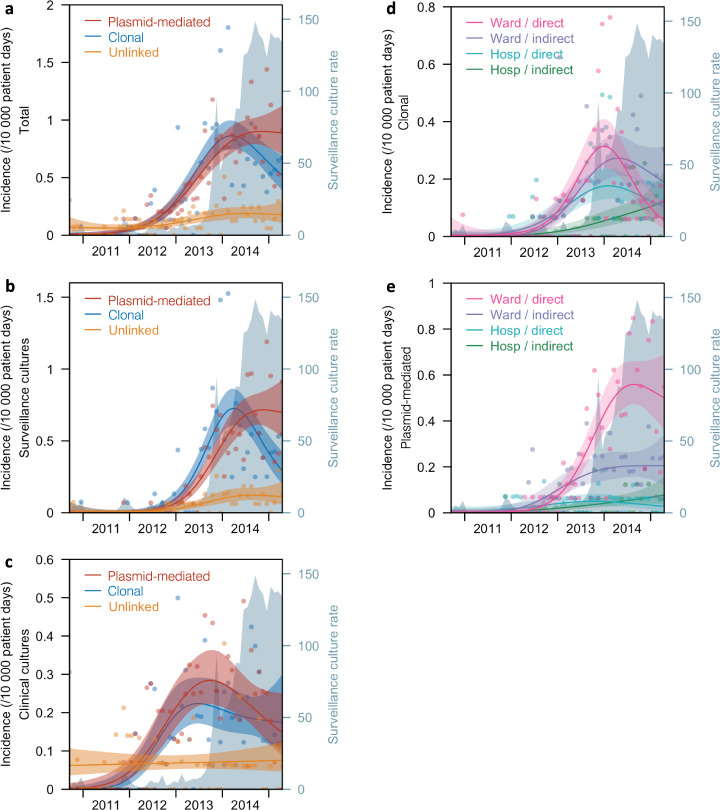
Carbapenemase-producing Enterobacterales (CPE) infection control practices are based on the paradigm that detected carriers in the hospital transmit to other patients who stay in the same ward. The role of plasmid-mediated transmission at population level remains largely unknown. In this retrospective cohort study over 4.7 years involving all multi-disciplinary public hospitals in Singapore, we analysed 779 patients who acquired CPE (1215 CPE isolates) detected by clinical or surveillance cultures. 42.0% met putative clonal transmission criteria, 44.8% met putative plasmid-mediated transmission criteria and 13.2% were unlinked. Only putative clonal transmissions associated with direct ward contact decreased in the second half of the study. Both putative clonal and plasmid-mediated transmission associated with indirect (no temporal overlap in patients' admission period) ward and hospital contact did not decrease during the study period. Indirect ward and hospital contact were identified as independent risk factors associated with clonal transmission. In conclusion, undetected CPE reservoirs continue to evade hospital infection prevention measures. New measures are needed to address plasmid-mediated transmission, which accounted for 50% of CPE dissemination.
© 2022. The Author(s).
Conflict of interest statement
D.W.E. declares personal fees from Gilead outside of the submitted work. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
