

The impact of ultra-high-density mapping on long-term outcome after catheter ablation of ventricular tachycardia
- PMID: 35650230
- PMCID: PMC9160260
- DOI: 10.1038/s41598-022-12918-7
The impact of ultra-high-density mapping on long-term outcome after catheter ablation of ventricular tachycardia
Abstract
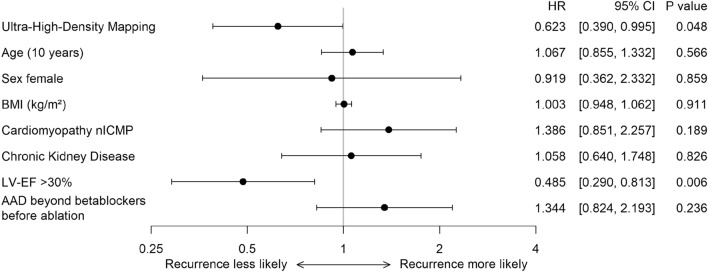
Ultra-high-density (UHD) mapping can improve scar area detection and fast activation mapping in patients undergoing catheter ablation of ventricular tachycardia (VT). The aim of the present study was to compare the outcome after VT ablation guided by UHD and conventional point-by-point 3D-mapping. The acute and long-term ablation outcome of 61 consecutive patients with UHD mapping (64-electrode mini-basket catheter) was compared to 61 consecutive patients with conventional point-by-point 3D-mapping using a 3.5 mm tip catheter. Patients, whose ablation was guided by UHD mapping had an improved 24-months outcome in comparison to patients with conventional mapping (cumulative incidence estimate of the combination of recurrence or disease-related death of 52.4% (95% confidence interval (CI) [36.9-65.7]; recurrence: n = 25; disease-related death: n = 4) versus 69.6% (95% CI [55.9-79.8]); recurrence: n = 31; disease-related death n = 11). In a cause-specific Cox proportional hazards model, UHD mapping (hazard ratio (HR) 0.623; 95% CI [0.390-0.995]; P = 0.048) and left ventricular ejection fraction > 30% (HR 0.485; 95% CI [0.290-0.813]; P = 0.006) were independently associated with lower rates of recurrence or disease-related death. Other procedural parameters were similar in both groups. In conclusion, UHD mapping during VT ablation was associated with fewer VT recurrences or disease-related deaths during long-term follow-up in comparison to conventional point-by-point mapping. Complication rates and other procedural parameters were similar in both groups.
© 2022. The Author(s).
Conflict of interest statement
C. Meyer, S. Willems, P. Jaïs, F. Sacher, H. Estner, C. Martin report honoraria as consultants or speaker’s fees relevant to this topic. The remaining authors declare no conflict of interests.
Figures



References
-
- Al-Khatib, S. M., Stevenson, W. G., Ackerman, M. J. et al. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm e73-e189 (2018). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
