

Communicating doctors' consensus persistently increases COVID-19 vaccinations
- PMID: 35650433
- PMCID: PMC9200639
- DOI: 10.1038/s41586-022-04805-y
Communicating doctors' consensus persistently increases COVID-19 vaccinations
Abstract
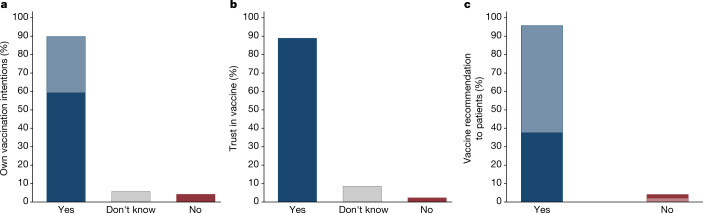
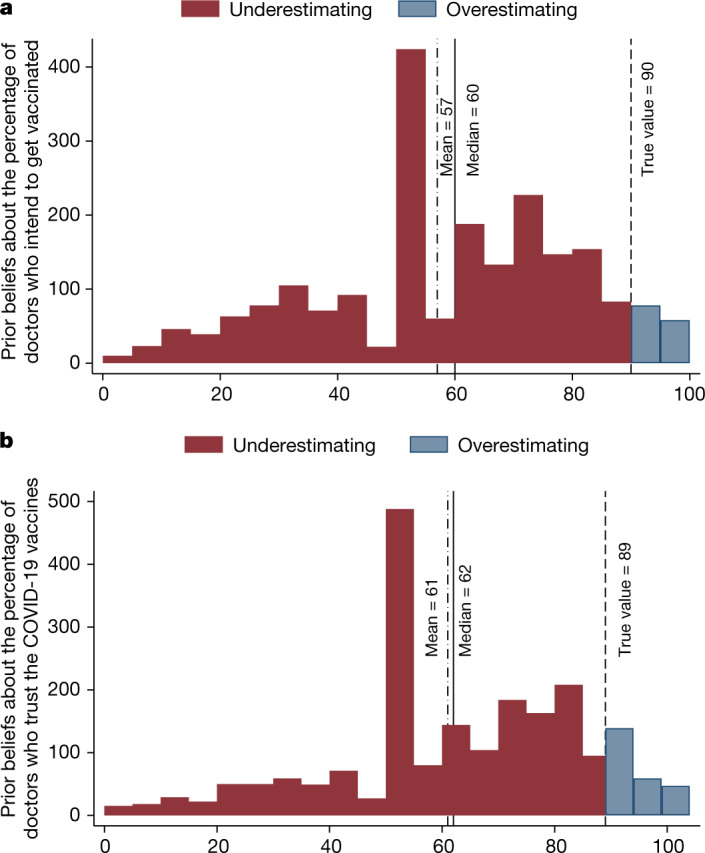
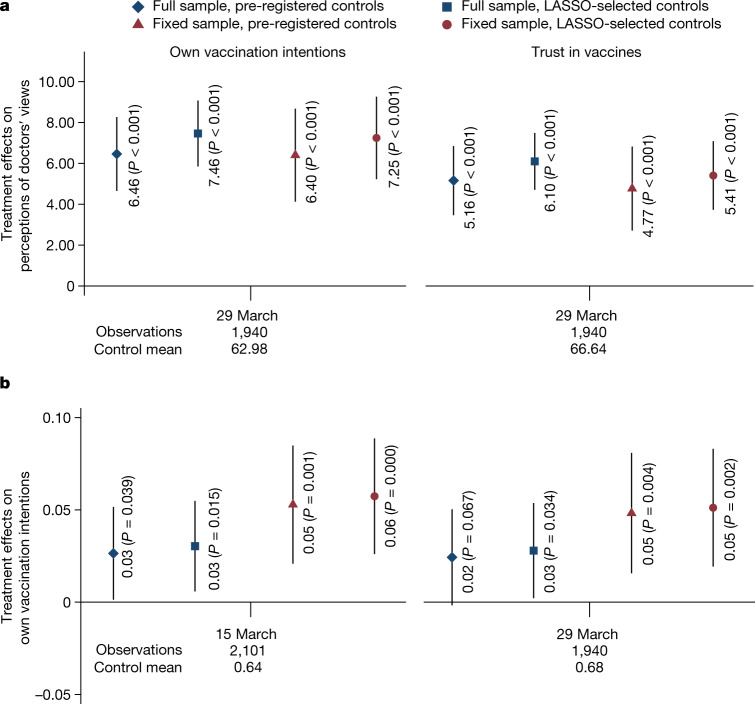
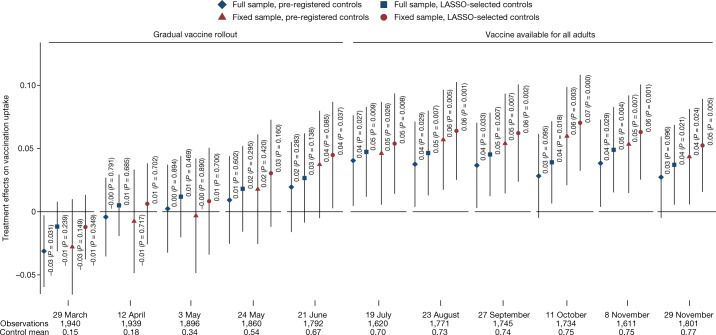
The reluctance of people to get vaccinated represents a fundamental challenge to containing the spread of deadly infectious diseases1,2, including COVID-19. Identifying misperceptions that can fuel vaccine hesitancy and creating effective communication strategies to overcome them are a global public health priority3-5. Medical doctors are a trusted source of advice about vaccinations6, but media reports may create an inaccurate impression that vaccine controversy is prevalent among doctors, even when a broad consensus exists7,8. Here we show that public misperceptions about the views of doctors on the COVID-19 vaccines are widespread, and correcting them increases vaccine uptake. We implement a survey among 9,650 doctors in the Czech Republic and find that 90% of doctors trust the vaccines. Next, we show that 90% of respondents in a nationally representative sample (n = 2,101) underestimate doctors' trust; the most common belief is that only 50% of doctors trust the vaccines. Finally, we integrate randomized provision of information about the true views held by doctors into a longitudinal data collection that regularly monitors vaccination status over 9 months. The treatment recalibrates beliefs and leads to a persistent increase in vaccine uptake. The approach demonstrated in this paper shows how the engagement of professional medical associations, with their unparalleled capacity to elicit individual views of doctors on a large scale, can help to create a cheap, scalable intervention that has lasting positive impacts on health behaviour.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Give physicians' views to improve COVID vaccine uptake.Nature. 2022 Jun;606(7914):471-472. doi: 10.1038/d41586-022-01305-x. Nature. 2022. PMID: 35650396 No abstract available.
References
-
- Banerjee, A. et al. Selecting the Most Effective Nudge: Evidence from a Large-Scale Experiment on Immunization. Working Paper 28726 (NBER, 2021).
