

Effect of specific training course for competency in professional oral hygiene care in the intensive care unit: a quasi-experimental study for developing a standardized learning curve
- PMID: 35650528
- PMCID: PMC9158265
- DOI: 10.1186/s12871-022-01709-2
Effect of specific training course for competency in professional oral hygiene care in the intensive care unit: a quasi-experimental study for developing a standardized learning curve
Abstract
Background: The development of evidence-based training standards can help improve the quality of educational programs for novice intensive care unit (ICU) nurses. This study was conducted to assess the application of a training course on competency development of nurses in relation to oral hygiene care in ICU patients and to develop a checklist for evaluating the competence performance. In addition, to achieve a certain level of oral hygiene competence, as well as to assess the relative importance of predicting factors and learning competency patterns in oral hygiene care, we used standard learning curve.
Methods: This quasi-experimental study with time series design was conducted on newly registered ICU nurses of a teaching hospital affiliated with Tehran University of Medical Sciences, Iran, between 2016 and 2018. In the first phase of this study, we designed a checklist to assess nurses' professional competence in oral hygiene care in three stages: before, during, and after care. Then, in the second phase, the level of competence of nurses in repeated times of oral hygiene care was determined based on checklist items and recorded in the learning curve.
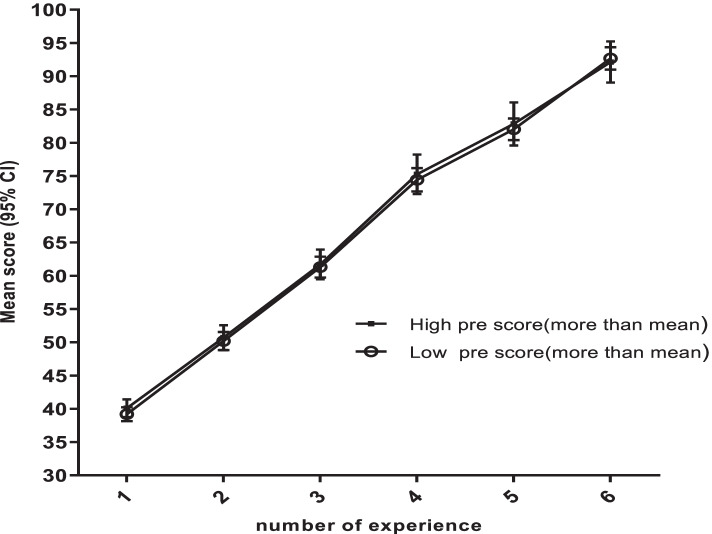
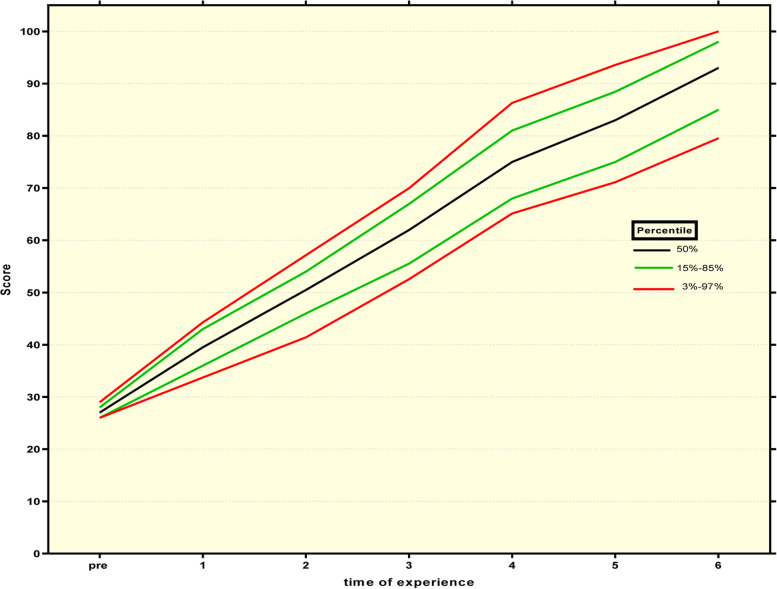
Results: The greatest increase of oral hygiene care competency due to repetition was observed in the first and fourth times of repetition in comparison to the subsequent and previous steps. In the linear regression model, demographic variables predicted 12-19% of changes related to skill scores in repetitions.
Conclusion: According to the learning curve, newly registered ICU nurses can reach an acceptable competency after 6 repetitions of oral hygiene care.
Keywords: Intensive care unit; Learning curve; Nursing education; Oral hygiene care.
© 2022. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to disclose related to this study.
Figures





References
-
- Recio-Saucedo A, Dall'Ora C, Maruotti A, Ball J, Briggs J, Meredith P, Redfern OC, Kovacs C, Prytherch D, Smith GB, et al. What impact does nursing care left undone have on patient outcomes? Review of the literature. J Clin Nurs. 2018;27(11–12):2248–2259. doi: 10.1111/jocn.14058. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
