

Impact of vaccine hesitancy on secondary COVID-19 outbreaks in the US: an age-structured SIR model
- PMID: 35650539
- PMCID: PMC9156621
- DOI: 10.1186/s12879-022-07486-0
Impact of vaccine hesitancy on secondary COVID-19 outbreaks in the US: an age-structured SIR model
Abstract
Background: The COVID-19 outbreak has become the worst pandemic in at least a century. To fight this disease, a global effort led to the development of several vaccines at an unprecedented rate. There have been, however, several logistic issues with its deployment, from their production and transport, to the hesitancy of the population to be vaccinated. For different reasons, an important amount of individuals is reluctant to get the vaccine, something that hinders our ability to control and-eventually-eradicate the disease.
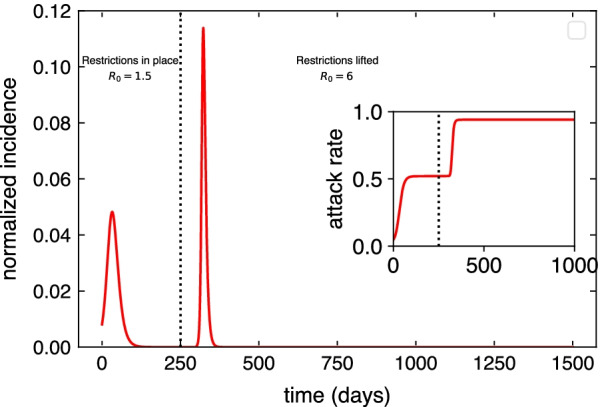
Materials and methods: Our aim is to explore the impact of vaccine hesitancy when highly transmissible SARS-CoV-2 variants of concern spread through a partially vaccinated population. To do so, we use age-stratified data from surveys on vaccination acceptance, together with age-contact matrices to inform an age-structured SIR model set in the US.
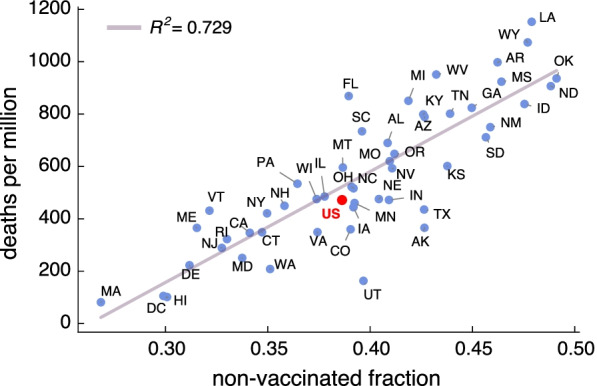
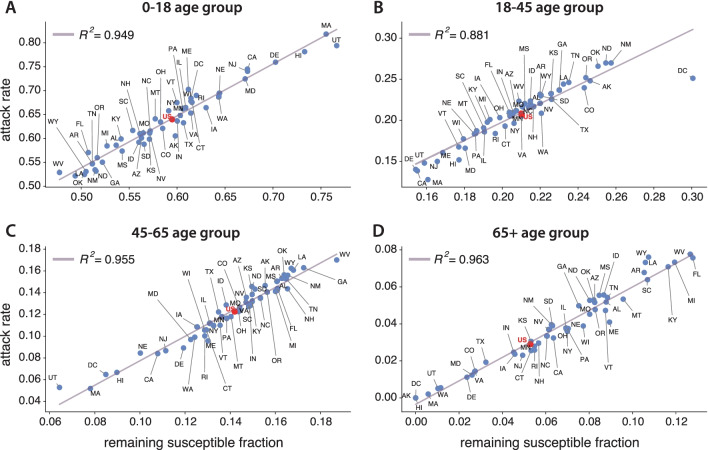
Results: Our results show that per every one percent decrease in vaccine hesitancy up to 45 deaths per million inhabitants could be averted. A closer inspection of the stratified infection rates also reveals the important role played by the youngest groups. The model captures the general trends of the Delta wave spreading in the US (July-October 2021) with a correlation coefficient of [Formula: see text].
Conclusions: Our results shed light on the role that hesitancy plays on COVID-19 mortality and highlight the importance of increasing vaccine uptake in the population, specially among the eldest age groups.
Keywords: Age-structured SIR; COVID-19; Hesitancy; Mathematical modeling; Vaccination.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
