

Labor induction in China: a nationwide survey
- PMID: 35650545
- PMCID: PMC9158355
- DOI: 10.1186/s12884-022-04760-6
Labor induction in China: a nationwide survey
Abstract
Background: Overmedicalization in labor management and delivery, including labor induction, is an increasing global concern. But detailed epidemiological data on labor induction in China remains unclear.
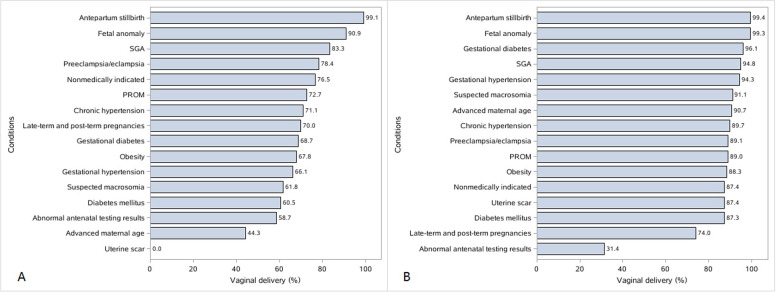
Methods: This was a cross-sectional study of data (2015-2016) from 96 hospitals in 24 (of 34) Chinese administrative divisions. Multivariable logistic regression analysis was used to assess the association between medical conditions and cesarean delivery among women undergoing induction. Linear regression analysis was performed to assess the association between the prelabor cesarean delivery and labor-induction rates in each hospital. The impacts of labor induction and prelabor cesarean delivery on maternal and neonatal outcomes were compared in low-risk women.
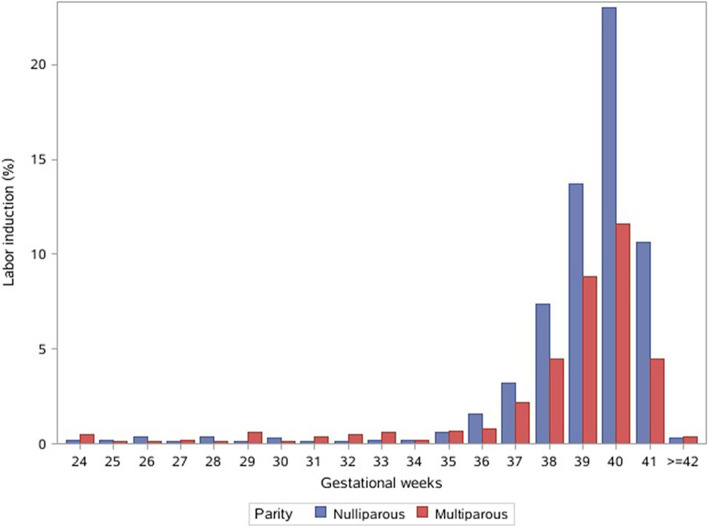
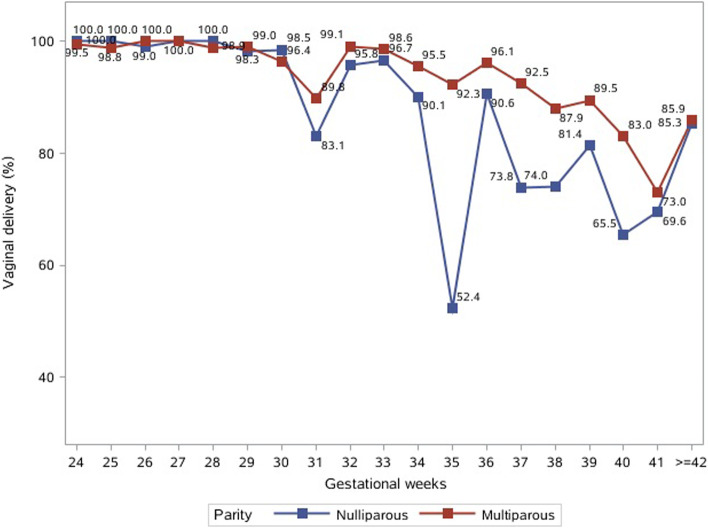
Results: Among 73 901 eligible participants, 48.1% were nulliparous. The overall weighted rate of labor induction in China was 14.2% (95% CI, 11.1-17.2%), with 18.4% (95% CI, 14.5-22.3%) in nulliparas and 10.2% (95% CI, 7.7-12.8%) in multiparas. Regardless of the induction method, the overall vaginal delivery rate was 72.9% (95% CI, 68.6-77.3%) in nulliparas and 86.6% (95% CI, 79.7-93.5%) in multiparas. Hospitals with a higher rate of nonmedically indicated cesarean delivery had a lower labor-induction rate in nulliparas (β = - 0.57%; 95% CI, - 0.92 to - 0.22%; P = 0.002). Compared with prelabor cesarean delivery, labor induction in low-risk women was not associated with adverse maternal and neonatal outcomes.
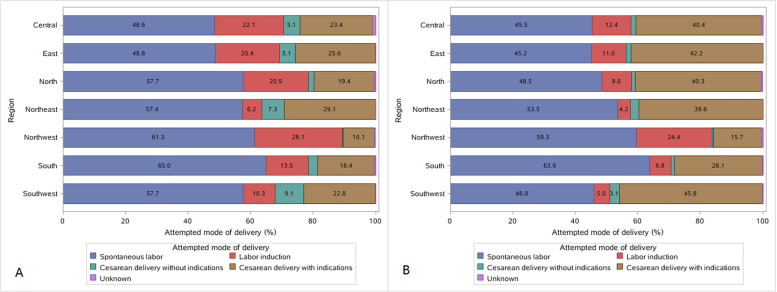
Conclusion: The 2015-2016 labor-induction rate in China was 18.4% in nulliparas and 10.2% in multiparas. The proportion of prelabor cesarean delivery may contribute to regional differences in the labor-induction rate. Compared with prelabor cesarean delivery, labor induction in low-risk women may not increase severe maternal and neonatal morbidity.
Keywords: Epidemiology; Labor induction; Obstetrics.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization. WHO recommendations for induction of labour. Geneva, Switzerland. 2011. http://whqlibdoc.who.int/hq/2011/WHO_RHR_11.10_eng.pdf - PubMed
-
- ACOG Committee on Practice Bulletins -- Obstetrics ACOG practice bulletin No. 107: induction of labor. Obstet Gynecol. 2009;114(2 Pt 1):386–97. - PubMed
-
- The National Institute for Health and Care Excellence. Inducing labor. NICE Guideline NG207; 2021. www.nice.org.uk/guidance/ng207.
-
- Gibbons L, Belizán JM, Lauer Ja, Betrán AP, Merialdi M, Althabe F. The global numbers and costs of additionally needed and unnecessary caesarean sections performed per year: overuse as a barrier to universal coverage. World Heal Rep Backgr Pap. 2010;30:1–31.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
