

Effective methods to enhance medical students' cardioversion and transcutaneous cardiac pacing skills retention - a prospective controlled study
- PMID: 35650577
- PMCID: PMC9158220
- DOI: 10.1186/s12909-022-03495-4
Effective methods to enhance medical students' cardioversion and transcutaneous cardiac pacing skills retention - a prospective controlled study
Abstract
Background: Guideline-based therapy of cardiac arrhythmias is important for many physicians from the beginning of their training. Practical training of the required skills to treat cardiac arrhythmias is useful for acquiring these skills but does not seem sufficient for skill retention. The aim of this study was to compare different retention methods for skills required to treat cardiac arrhythmias with respect to the performance of these skills in an assessment.
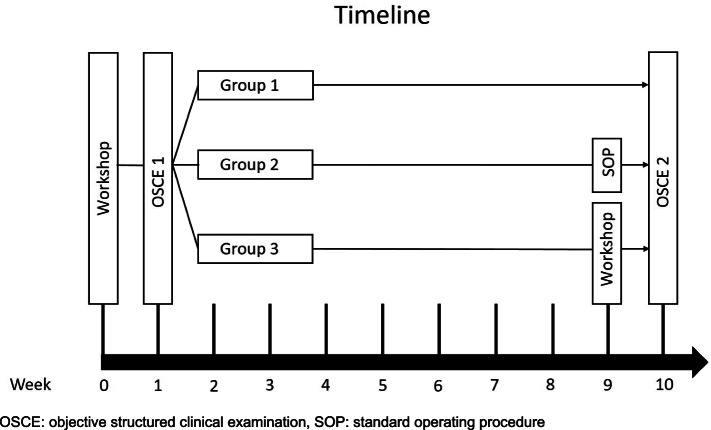
Methods: Seventy-one final-year medical students participated in a newly designed workshop to train synchronized cardioversion (SC) and transcutaneous cardiac pacing (TCP) skills in 2020. All participants completed an objective structured clinical examination (OSCE 1) one week after the training. Afterwards, the participants were stratified and randomized into three groups. Nine weeks later, one group received a standard operating procedure (SOP) for the skills, one group participated in a second workshop (SW), and one group received no further intervention (control). Ten weeks after the first training, all groups participated in OSCE 2.
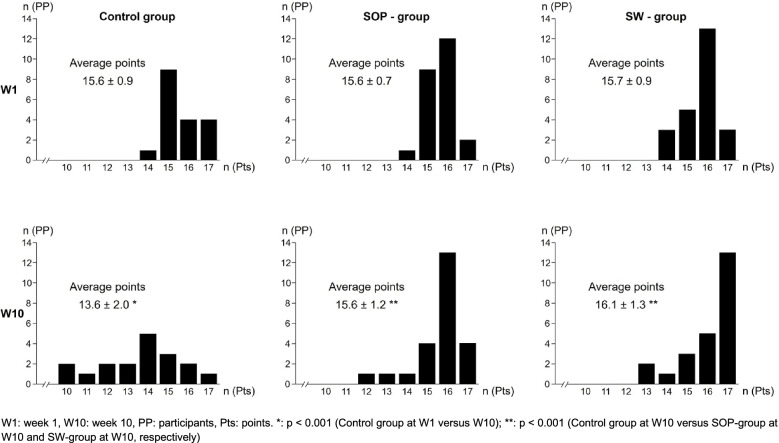
Results: The average score of all students in OSCE 1 was 15.6 ± 0.8 points with no significant differences between the three groups. Students in the control group reached a significantly (p < 0.001) lower score in OSCE 2 (-2.0 points, CI: [-2.9;-1.1]) than in OSCE 1. Students in the SOP-group achieved on average the same result in OSCE 2 as in OSCE 1 (0 points, CI: [-0.63;+0.63]). Students who completed a second skills training (SW-group) scored not significantly higher in OSCE 2 compared to OSCE 1 (+0.4 points, CI: [-0.29;+1.12]). The OSCE 2 scores in groups SOP and SW were neither significantly different nor statistically equivalent.
Conclusions: Partial loss of SC and TCP skills acquired in a workshop can be prevented after 10 weeks by reading an SOP as well as by a second workshop one week before the second assessment. Refreshing practical skills with an SOP could provide an effective and inexpensive method for skills retention compared to repeating a training. Further studies need to show whether this effect also exists for other skills and how frequently an SOP should be re-read for appropriate long-term retention of complex skills.
Keywords: Objective structured clinical examination (OSCE); Performance; Skill retention; Skills training; Standard operating procedure (SOP); Synchronized cardioversion; Transcutaneous pacing.
© 2022. The Author(s).
Conflict of interest statement
SH has a position as Senior Editorial Board Member to BMC Medical Education. CK and AB have no competing interests.
Figures
References
-
- Robitaille A, Perron R, Germain JF, Tanoubi I, Georgescu M. High-fidelity simulation of transcutaneous cardiac pacing - characteristics and limitations of available high-fidelity simulators, and description of an alternative two-mannequin model. Sim Healthc. 2015;10:122–127. doi: 10.1097/SIH.0000000000000067. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
