

The Clinical Course of Early and Late Mild Cognitive Impairment
- PMID: 35651352
- PMCID: PMC9149311
- DOI: 10.3389/fneur.2022.685636
The Clinical Course of Early and Late Mild Cognitive Impairment
Abstract
Introduction: Amnestic mild cognitive impairment (MCI) can be classified as either early MCI (EMCI) or late MCI (LMCI) according to the severity of memory impairment. The aim of this study was to compare the prognosis and clinical course between EMCI and LMCI.
Methods: Between January 2009 and December 2017, a total of 418 patients with MCI and 146 subjects with normal cognition were recruited from a memory clinic. All the patients received at least two series of neuropsychological evaluations each year and were categorized as either EMCI or LMCI according to Alzheimer's Disease Neuroimaging Initiative 2 (ADNI2) criteria.
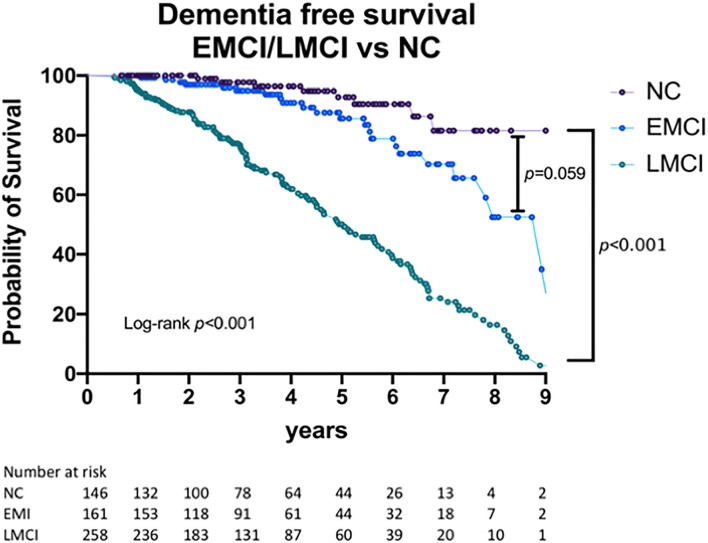
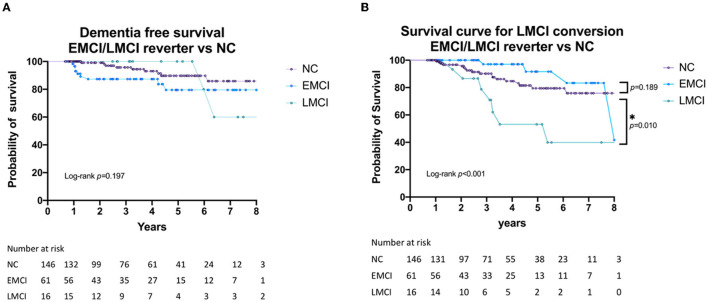
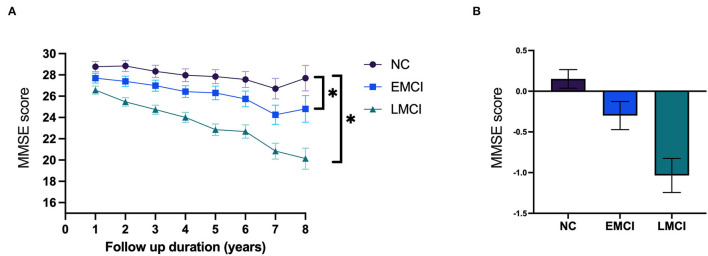
Results: In total, our study included 161 patients with EMCI, 258 with LMCI, and 146 subjects with normal cognition as controls (NCs). The mean follow-up duration was 3.55 ± 2.18 years (range: 1-9). In a first-year follow-up assessment, 54 cases (32.8%) of EMCI and 16 (5%) of LMCI showed a normal cognitive status. There was no significant difference between the first year EMCI reverter and NCs in terms of dementia-free survival and further cognitive decline. However, first-year LMCI reverters still had a higher risk of cognitive decline during the following evaluations. Until the last follow-up, annual dementia conversion rates were 1.74, 4.33, and 18.6% in the NC, EMCI, and LMCI groups, respectively. The EMCI and LMCI groups showed a higher rate of progression to dementia (log-rank test, p < 0.001) than normal subjects. Compared with NCs, patients in the LMCI group showed a significantly faster annual decline in global cognition [annual rate of change for the mini-mental status examination (MMSE) score: -1.035, p < 0.001]) and all cognitive domains, while those in the EMCI group showed a faster rate of decline in global cognitive function (annual rate of change for the MMSE score: -0.299, p = 0.001).
Conclusion: It is important to arrange follow-up visits for patients with MCI, even in the EMCI stage. One-year short-term follow-up may provide clues about the progression of cognitive function and help to identify relatively low-risk EMCI subjects.
Keywords: Alzheimer's Disease; cognitive tests; early mild cognitive impairment (EMCI); longitudinal follow-up; mild cognitive impairment (MCI).
Copyright © 2022 Lin, Lin, Lin, Lee, Wang, Peng and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Lee E-S, Yoo K, Lee Y-B, Chung J, Lim J-E, Yoon B, et al. . Default mode network functional connectivity in early and late mild cognitive impairment: results from the alzheimer's disease neuroimaging initiative. Alzheimer Dis Assoc Disord. (2016) 30:289–96. 10.1097/WAD.0000000000000143 - DOI - PubMed
LinkOut - more resources
Full Text Sources