

Ventilation Liberation Practices Among 380 International PICUs
- PMID: 35651738
- PMCID: PMC9150886
- DOI: 10.1097/CCE.0000000000000710
Ventilation Liberation Practices Among 380 International PICUs
Abstract
1) Characterize the prevalence of ventilator liberation protocol use in international PICUs, 2) identify the most commonly used protocol elements, and 3) estimate an international extubation failure rate and use of postextubation noninvasive respiratory support modes.
Design: International cross-sectional study.
Subjects: Nontrainee pediatric medical and cardiac critical care physicians.
Setting: Electronic survey.
Intervention: None.
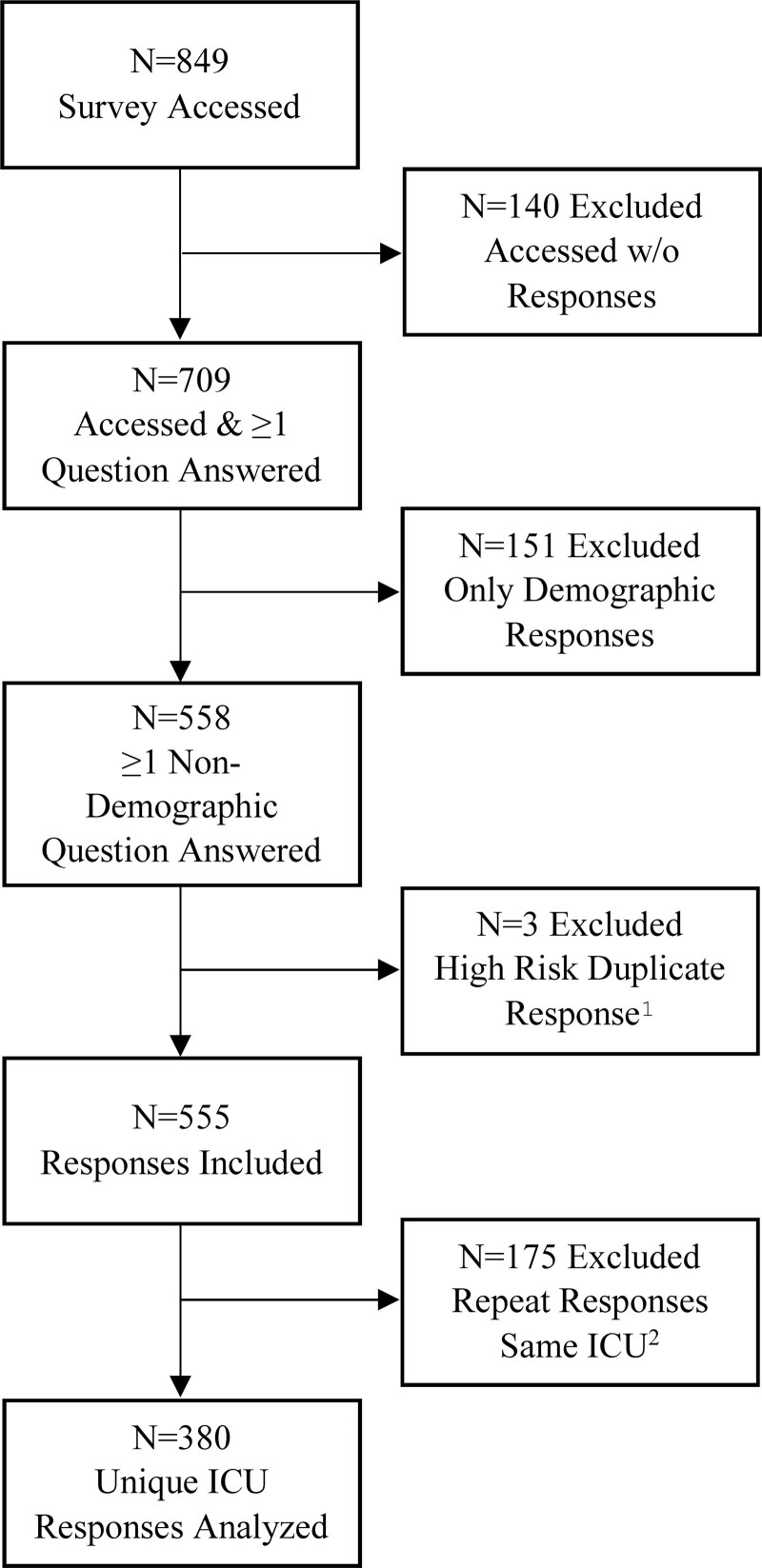
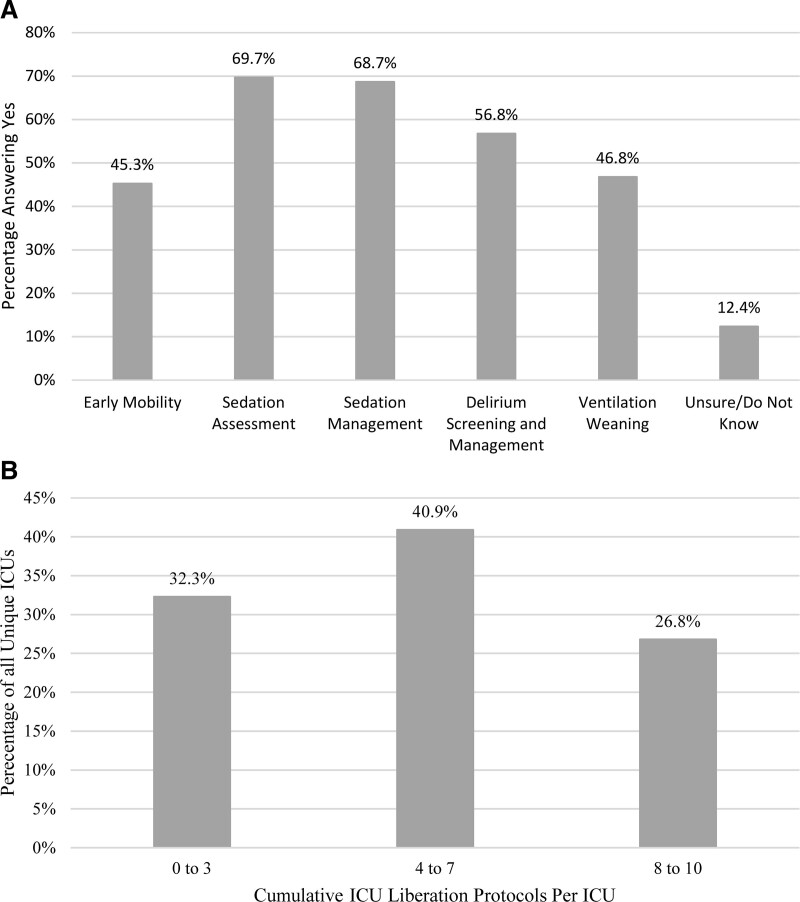
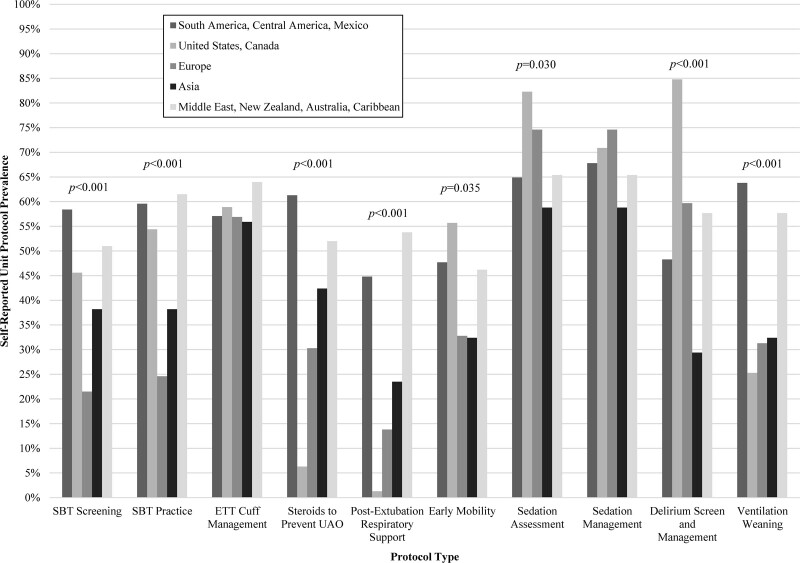
Measurements and main results: Responses represented 380 unique PICUs from 47 different countries. Protocols for Spontaneous Breathing Trial (SBT) practice (50%) and endotracheal tube cuff management (55.8%) were the only protocols used by greater than or equal to 50% of PICUs. Among PICUs screening for SBT eligibility, physicians were most commonly screened (62.7%) with daily frequency (64.2%). Among those with an SBT practice protocol, SBTs were most commonly performed by respiratory therapists/physiotherapists (49.2%) and least commonly by nurses (4.9%). Postextubation respiratory support protocols were not prevalent (28.7%). International practice variation was significant for most practices surveyed. The estimated median international extubation failure was 5% (interquartile range, 2.3-10%). A majority of respondents self-reported use of planned high-flow nasal cannula in less than or equal to 50% (84.2%) and planned noninvasive ventilation in less than or equal to 20% of extubations (81.6%).
Conclusions: Variability in international pediatric ventilation liberation practice is high, and prevalence of protocol implementation is generally low. There is a need to better understand elements that drive clinical outcomes and opportunity to work on standardizing pediatric ventilation liberation practices worldwide.
Keywords: clinical pathway; extubation; mechanical ventilation; pediatric intensive care unit; pediatrics; respiratory therapy.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Ely EW, Baker AM, Dunagan DP, et al. : Effect on the duration of mechanical ventilation of identifying patients capable of breathing spontaneously. N Engl J Med 1996; 335:1864–1869 - PubMed
-
- Farias JA, Retta A, Alía I, et al. : A comparison of two methods to perform a breathing trial before extubation in pediatric intensive care patients. Intensive Care Med 2001; 27:1649–1654 - PubMed
-
- Foronda FK, Troster EJ, Farias JA, et al. : The impact of daily evaluation and spontaneous breathing test on the duration of pediatric mechanical ventilation: A randomized controlled trial. Crit Care Med 2011; 39:2526–2533 - PubMed
LinkOut - more resources
Full Text Sources
