

Assessment of New Onset Arrhythmias After Transcatheter Aortic Valve Implantation Using an Implantable Cardiac Monitor
- PMID: 35651903
- PMCID: PMC9149277
- DOI: 10.3389/fcvm.2022.876546
Assessment of New Onset Arrhythmias After Transcatheter Aortic Valve Implantation Using an Implantable Cardiac Monitor
Abstract
Background: Transcatheter aortic valve implantation (TAVI) is associated with new onset brady- and tachyarrhythmias which may impact clinical outcome.
Aims: To investigate the true incidence of new onset arrhythmias within 12 months after TAVI using an implantable cardiac monitor (ICM).
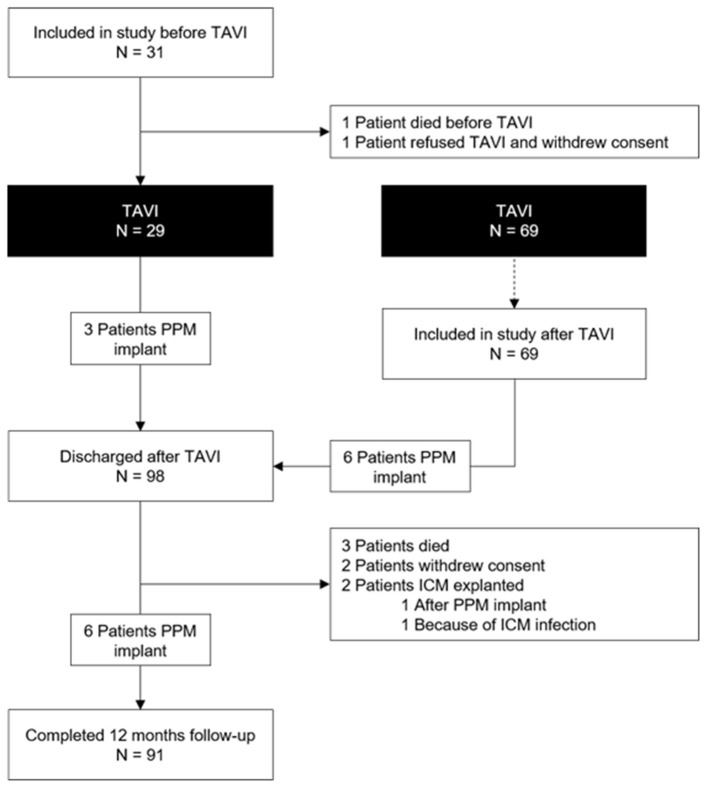
Methods: One hundred patients undergoing TAVI received an ICM within 3 months before or up to 5 days after TAVI. Patients were followed-up for 12 months after discharge from TAVI for the occurrence of atrial fibrillation (AF), bradycardia (≤30 bpm), advanced atrioventricular (AV) block, sustained ventricular and supraventricular tachycardia.
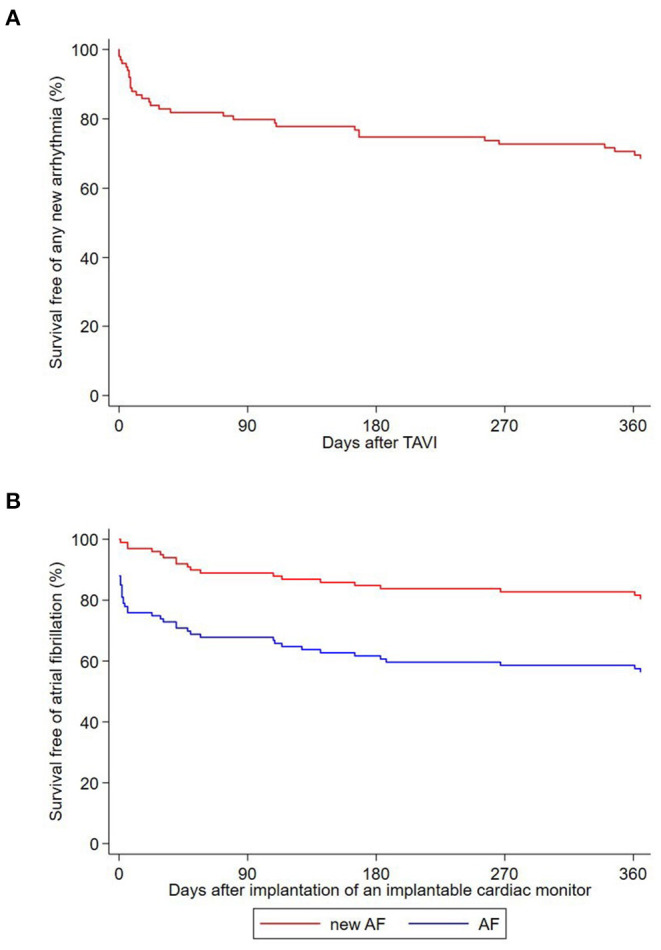
Results: A previously undiagnosed arrhythmia was observed in 31 patients (31%) and comprised AF in 19 patients (19%), advanced AV block in 3 patients (3%), and sustained supraventricular and ventricular tachycardia in 10 (10%) and 2 patients (2%), respectively. Three patients had a clinical diagnosis of sick-sinus-syndrome. A permanent pacemaker (PPM) was implanted in six patients (6%). The prevalence of pre-existing AF was 28%, and 47% of the patients had AF at the end of the study period. AF burden was significantly higher in patients with pre-existing [26.7% (IQR 0.3%; 100%)] compared to patients with new-onset AF [0.0% (IQR 0.0%; 0.06%); p = 0.001]. Three patients died after TAVI without evidence of an arrhythmic cause according to the available ICM recordings.
Conclusions: Rhythm monitoring for 12 months after TAVI revealed new arrhythmias, mainly AF, in almost one third of patients. Atrial fibrillation burden was higher in patients with prevalent compared to incident AF. Selected patients may benefit from short-term remote monitoring.
Trial registration: https://clinicaltrials.gov/: NCT02559011.
Keywords: AV block; TAVI; atrial fibrillation; bundle branch block (BBB); implantable cardiac monitor (ICM); pacemaker (PM); ventricular tachycardia (VT).
Copyright © 2022 Nozica, Siontis, Elchinova, Goulouti, Asami, Bartkowiak, Baldinger, Servatius, Seiler, Tanner, Noti, Haeberlin, Branca, Lanz, Stortecky, Pilgrim, Windecker, Reichlin, Praz and Roten.
Conflict of interest statement
The spouse of JS is an employee of Boston Scientific. HT reports educational grants from Biosense Webster and travel grants from Abbott. FN reports travel fees from Medtronic, Abbott, Boston Scientific and Philips Spectranetics, speaker fees from Medtronic and Abbott, educational grants from Medtronic, Abbott, Boston Scientific, Philips Spectranetics and Actinno and institutional grants from Biotronik. AH received travel/educational grants from Medtronic and Philips/Spectranetics. He is consultant/advisor for DiNAQOR and Biotronik and Co-founder/head of Act-Inno. SS reports research grants to the institution from Edwards Lifesciences, Medtronic, Boston Scientific and Abbott, as well as personal fees from Boston Scientific, Teleflex and BTG. TP reports research grants to the institution from Biotronik, Boston Scientific and Edwards Lifesciences; speaker fees from Biotronik and Boston Scientific; Clinical event committee for study sponsored by HighLifeSAS; travel reimbursement from Medira; proctoring for Medtronic. SW reports research and educational grants to the institution from Abbott, Amgen, Astra Zeneca, BMS, Bayer, Biotronik, Boston Scientific, Cardinal Health, CardioValve, CSL Behring, Daiichi Sankyo, Edwards Lifesciences, Guerbet, InfraRedx, Johnson & Johnson, Medicure, Medtronic, Novartis, Polares, OrPha Suisse, Pfizer, Regeneron, Sanofi-Aventis, Sinomed, Terumo, V-Wave. He serves as unpaid advisory board member and/or unpaid member of the steering/executive group of trials funded by Abbott, Abiomed, Amgen, Astra Zeneca, Bayer, BMS, Boston Scientific, Biotronik, Cardiovalve, Edwards Lifesciences, MedAlliance, Medtronic, Novartis, Polares, Sinomed, Terumo, V-Wave and Xeltis, but has not received personal payments by pharmaceutical companies or device manufacturers. He is also member of the steering/executive committee group of several investigator-initiated trials that receive funding by industry without impact on his personal remuneration. TR reported research grants from the Goldschmidt-Jacobson Foundation, the Swiss National Science Foundation, the Swiss Heart Foundation and the sitem-insel Support Funds, all for work outside the submitted study; advisory board membership, speaker and travel support from Abbott/SJM, Astra Zeneca, Brahms, Bayer, Biosense-Webster, Biotronik, Boston-Scientific, Daiichi Sankyo, Medtronic, Pfizer-BMS and Roche, all for work outside the submitted study and without impact on his personal remuneration; as well as support for his institution's fellowship program from Abbott/SJM, Biosense-Webster, Biotronik, Boston-Scientific and Medtronic for work outside the submitted study and without impact on his personal remuneration. FP reports travel expenses from Abbott Vascular, Edwards Lifesciences, and Polares Medical. LR received speaker honoraria from Abbott/SJM and consulting honoraria from Medtronic. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Mack MJ, Leon MB, Smith CR, Miller DC, Moses JW, Tuzcu EM, et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. (2015) 385:2477–84. 10.1016/S0140-6736(15)60308-7 - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical