

Troubleshooting Gait Disturbances in Parkinson's Disease With Deep Brain Stimulation
- PMID: 35652005
- PMCID: PMC9148971
- DOI: 10.3389/fnhum.2022.806513
Troubleshooting Gait Disturbances in Parkinson's Disease With Deep Brain Stimulation
Abstract
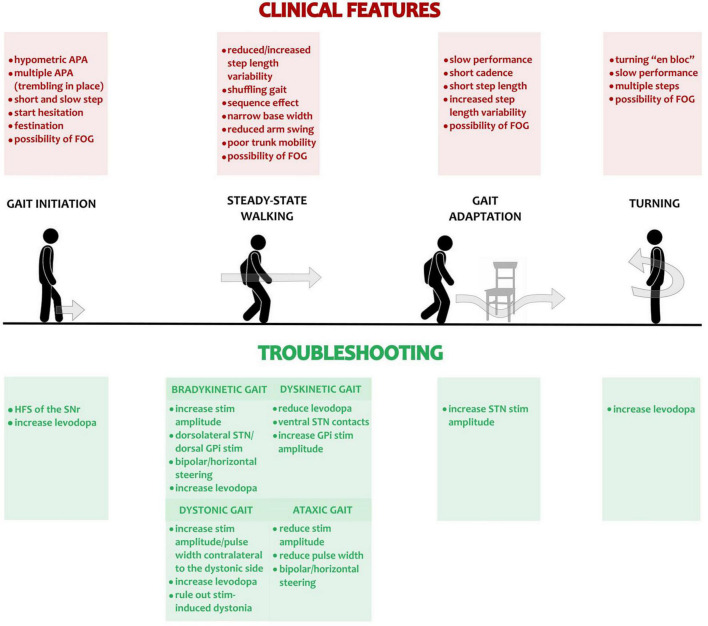
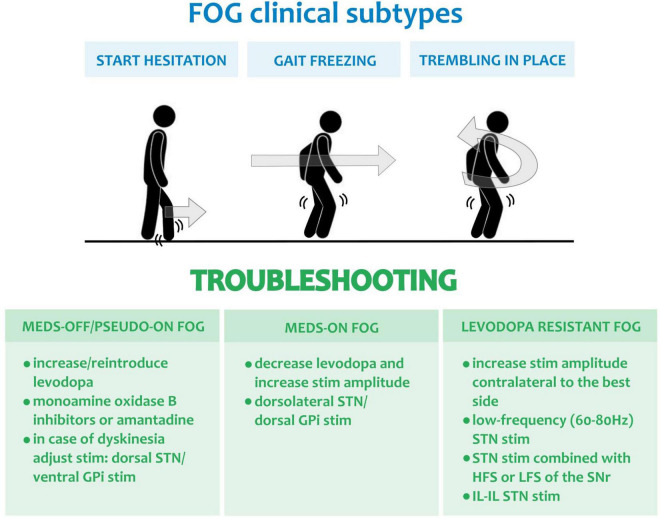
Deep brain stimulation (DBS) of the subthalamic nucleus or the globus pallidus is an established treatment for Parkinson's disease (PD) that yields a marked and lasting improvement of motor symptoms. Yet, DBS benefit on gait disturbances in PD is still debated and can be a source of dissatisfaction and poor quality of life. Gait disturbances in PD encompass a variety of clinical manifestations and rely on different pathophysiological bases. While gait disturbances arising years after DBS surgery can be related to disease progression, early impairment of gait may be secondary to treatable causes and benefits from DBS reprogramming. In this review, we tackle the issue of gait disturbances in PD patients with DBS by discussing their neurophysiological basis, providing a detailed clinical characterization, and proposing a pragmatic programming approach to support their management.
Keywords: Parkinson’s disease; deep brain stimulation (DBS); freezing of gait (FOG); globus pallidus pars interna (GPi); pedunculopontine nucleus (PPN); subthalamic nucleus (STN).
Copyright © 2022 Pozzi, Palmisano, Reich, Capetian, Pacchetti, Volkmann and Isaias.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Factors correlated with therapeutic effects of globus pallidus deep brain stimulation on freezing of gait in advanced Parkinson's disease: A pilot study.Parkinsonism Relat Disord. 2022 Jan;94:111-116. doi: 10.1016/j.parkreldis.2021.12.005. Epub 2021 Dec 10. Parkinsonism Relat Disord. 2022. PMID: 34915449
-
Effects of deep brain stimulation on balance and gait in patients with Parkinson's disease: A systematic neurophysiological review.Neurophysiol Clin. 2015 Nov;45(4-5):371-88. doi: 10.1016/j.neucli.2015.07.001. Epub 2015 Aug 28. Neurophysiol Clin. 2015. PMID: 26319759 Review.
-
Deep brain stimulation of globus pallidus interna, subthalamic nucleus, and pedunculopontine nucleus for Parkinson's disease: which target?Parkinsonism Relat Disord. 2012 Jan;18 Suppl 1:S165-7. doi: 10.1016/S1353-8020(11)70051-7. Parkinsonism Relat Disord. 2012. PMID: 22166422 Review.
-
Comparison of the Efficacy of Deep Brain Stimulation in Different Targets in Improving Gait in Parkinson's Disease: A Systematic Review and Bayesian Network Meta-Analysis.Front Hum Neurosci. 2021 Oct 22;15:749722. doi: 10.3389/fnhum.2021.749722. eCollection 2021. Front Hum Neurosci. 2021. PMID: 34744665 Free PMC article.
-
Deep brain stimulation of the subthalamic and pedunculopontine nucleus in a patient with Parkinson's disease.J Korean Neurosurg Soc. 2015 Apr;57(4):303-6. doi: 10.3340/jkns.2015.57.4.303. Epub 2015 Apr 24. J Korean Neurosurg Soc. 2015. PMID: 25932301 Free PMC article.
Cited by
-
Cortical networks of parkinsonian gait: a metabolic and functional connectivity study.Ann Clin Transl Neurol. 2024 Oct;11(10):2597-2608. doi: 10.1002/acn3.52173. Epub 2024 Aug 26. Ann Clin Transl Neurol. 2024. PMID: 39186320 Free PMC article.
-
Case report: Improvement of gait with adaptive deep brain stimulation in a patient with Parkinson's disease.Front Bioeng Biotechnol. 2024 Sep 11;12:1428189. doi: 10.3389/fbioe.2024.1428189. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 39323762 Free PMC article.
-
Gait-related beta-gamma phase amplitude coupling in the subthalamic nucleus of parkinsonian patients.Sci Rep. 2024 Mar 20;14(1):6674. doi: 10.1038/s41598-024-57252-2. Sci Rep. 2024. PMID: 38509158 Free PMC article.
-
Subthalamic 85 Hz deep brain stimulation improves walking pace and stride length in Parkinson's disease patients.Neurol Res Pract. 2023 Aug 10;5(1):33. doi: 10.1186/s42466-023-00263-7. Neurol Res Pract. 2023. PMID: 37559161 Free PMC article.
-
Modeling and optimizing deep brain stimulation to enhance gait in Parkinson's disease: personalized treatment with neurophysiological insights.NPJ Parkinsons Dis. 2025 Jun 18;11(1):173. doi: 10.1038/s41531-025-00990-5. NPJ Parkinsons Dis. 2025. PMID: 40533464 Free PMC article.
References
-
- Andreasi N. G., Rispoli V., Contaldi E., Colucci F., Mongardi L., Cavallo M. A., et al. (2020). Deep brain stimulation and refractory freezing of gait in Parkinson’s disease: improvement with high-frequency current steering co-stimulation of subthalamic nucleus and substantia Nigra. Brain Stimul. 13 280–283. 10.1016/J.BRS.2019.10.010 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous