

Ischemic stroke with cancer: Hematologic and embolic biomarkers and clinical outcomes
- PMID: 35652416
- PMCID: PMC9378694
- DOI: 10.1111/jth.15779
Ischemic stroke with cancer: Hematologic and embolic biomarkers and clinical outcomes
Abstract
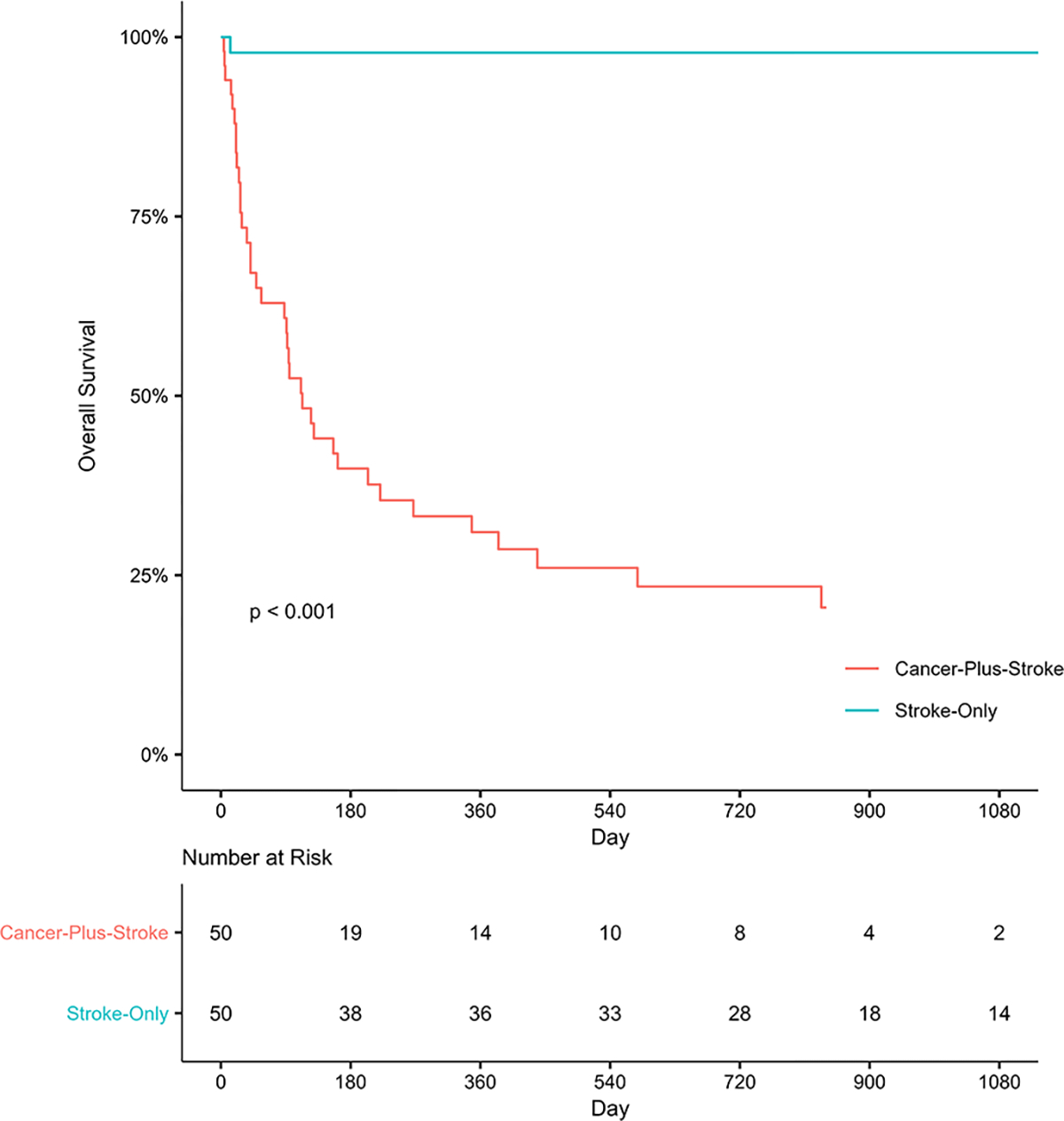
Background: Patients with cancer and acute ischemic stroke (AIS) face high rates of recurrent thromboembolism or death.
Objectives: To examine whether hematologic and embolic biomarkers soon after AIS are associated with subsequent adverse clinical outcomes.
Methods: We prospectively enrolled 50 adults with active solid tumor cancer and AIS at two hospitals from 2016 to 2020. Blood was collected 72-120 h after stroke onset. A 30-min transcranial Doppler (TCD) microemboli detection study was performed. The exposure variables were hematologic markers of coagulation (D-dimer, thrombin-antithrombin), platelet (P-selectin), and endothelial activation (thrombomodulin, soluble intercellular adhesion molecule-1 [sICAM-1], soluble vascular cell adhesion molecule-1 [sVCAM-1]), and the presence of TCD microemboli. The primary outcome was a composite of recurrent arterial/venous thromboembolism or death. We used Cox regression to evaluate associations between biomarkers and subsequent outcomes.
Results: During an estimated median follow-up time of 48 days (IQR, 18-312), 43 (86%) participants developed recurrent thromboembolism or death, including 28 (56%) with recurrent thromboembolism, of which 13 were recurrent AIS (26%). In unadjusted analysis, D-dimer (HR 1.6; 95% CI 1.2-2.0), P-selectin (HR 1.9; 95% CI 1.4-2.7), sICAM-1 (HR 2.2; 95% CI 1.6-3.1), sVCAM-1 (HR 1.6; 95% CI 1.2-2.1), and microemboli (HR 2.2; 95% CI 1.1-4.5) were associated with the primary outcome, whereas thrombin-antithrombin and thrombomodulin were not. D-dimer was the only marker associated with recurrent AIS (HR 1.2; 95% CI 1.0-1.5). Results were generally consistent in analyses adjusted for important prognostic variables.
Conclusions: Markers of hypercoagulability and embolic disease may be associated with adverse clinical outcomes in cancer-related stroke.
Keywords: biomarkers; neoplasms; stroke; thrombophilia; thrombosis.
© 2022 International Society on Thrombosis and Haemostasis.
Conflict of interest statement
Disclosures
Hooman Kamel, co-PI for the ARCADIA trial, has received in-kind study drug from BMS-Pfizer Alliance and in-kind study assays from Roche Diagnostics; serves as Deputy Editor for
Figures




References
-
- Navi BB, Howard G, Howard VJ, Zhao H, Judd SE, Elkind MSV, Iadecola C, DeAngelis LM, Kamel H, Okin PM, Gilchrist S, Soliman EZ, Cushman M, Muntner P. New diagnosis of cancer and the risk of subsequent cerebrovascular events. Neurology. 2018; 90: e2025–e33. 10.1212/WNL.0000000000005636. - DOI - PMC - PubMed
-
- Kiyuna F, Sato N, Matsuo R, Kamouchi M, Hata J, Wakisaka Y, Kuroda J, Ago T, Kitazono T, Fukuoka Stroke Registry I. Association of Embolic Sources With Cause-Specific Functional Outcomes Among Adults With Cryptogenic Stroke. JAMA Netw Open. 2018; 1: e182953. 10.1001/jamanetworkopen.2018.2953. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
