

Efficacy, Safety, and Tolerability of Centanafadine Sustained-Release Tablets in Adults With Attention-Deficit/Hyperactivity Disorder: Results of 2 Phase 3, Randomized, Double-blind, Multicenter, Placebo-Controlled Trials
- PMID: 35652746
- PMCID: PMC9426730
- DOI: 10.1097/JCP.0000000000001575
Efficacy, Safety, and Tolerability of Centanafadine Sustained-Release Tablets in Adults With Attention-Deficit/Hyperactivity Disorder: Results of 2 Phase 3, Randomized, Double-blind, Multicenter, Placebo-Controlled Trials
Abstract
Purpose/background: Centanafadine is an inhibitor of norepinephrine, dopamine, and serotonin reuptake transporters under investigation for the treatment of attention-deficit/hyperactivity disorder (ADHD).
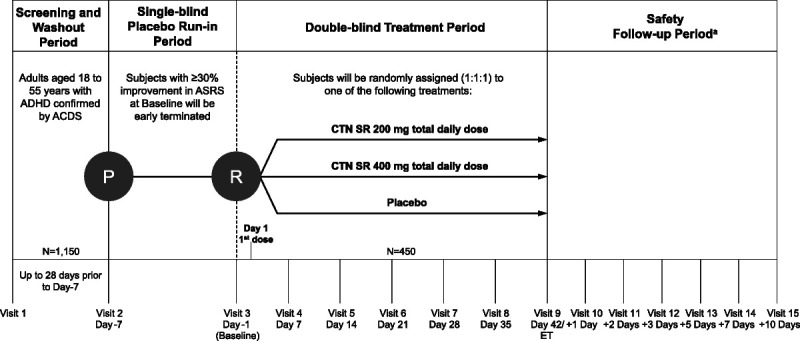
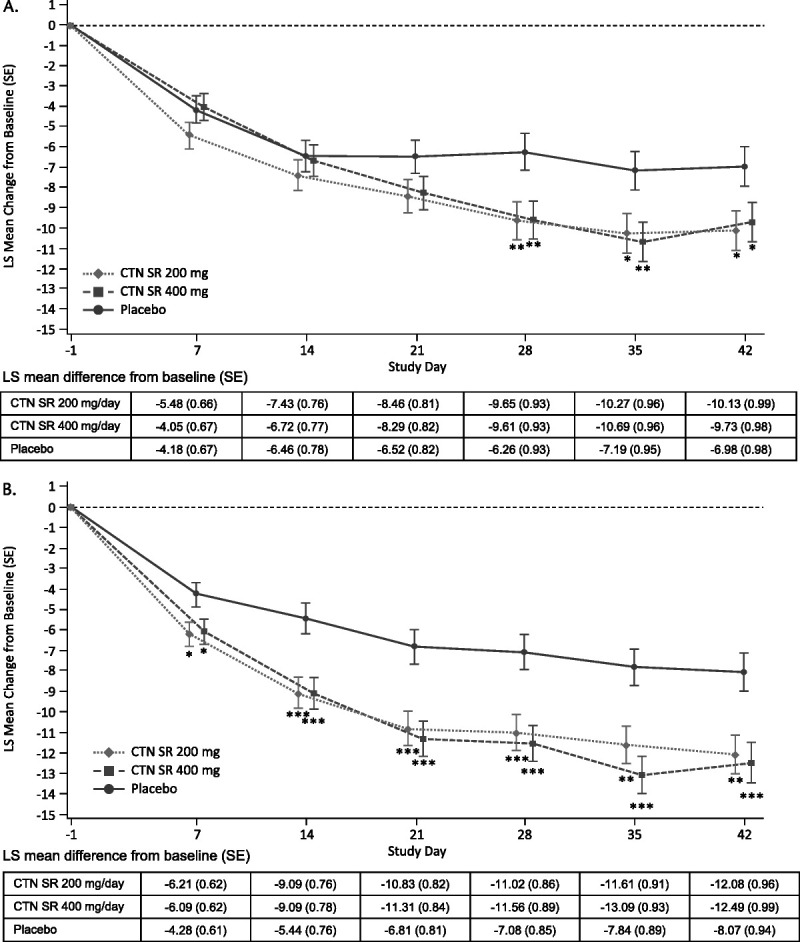
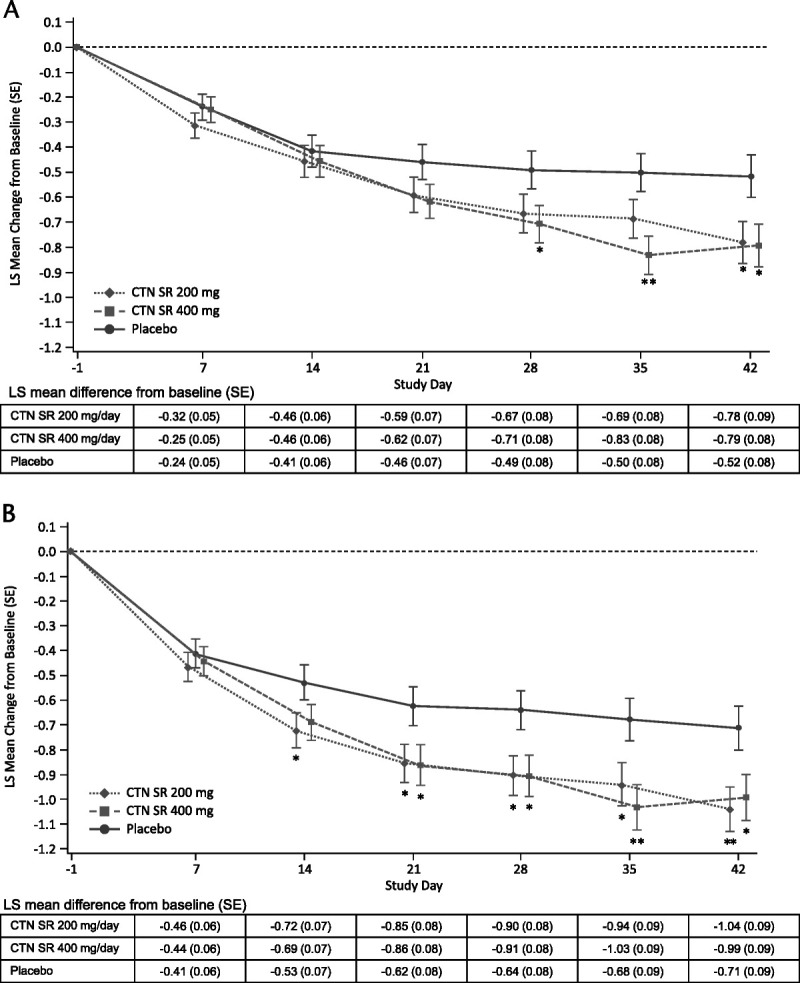
Methods/procedures: Two phase 3 randomized, double-blind, placebo-controlled, parallel-group studies of 200 mg/d or 400 mg/d centanafadine sustained-release tablets versus placebo included adults (18-55 years of age) with a diagnosis of ADHD. The primary and key secondary efficacy endpoints were the change from baseline at day 42 in the Adult ADHD Investigator Symptom Rating Scale (AISRS) total score and the Clinical Global Impression-Severity of Illness Scale, respectively.
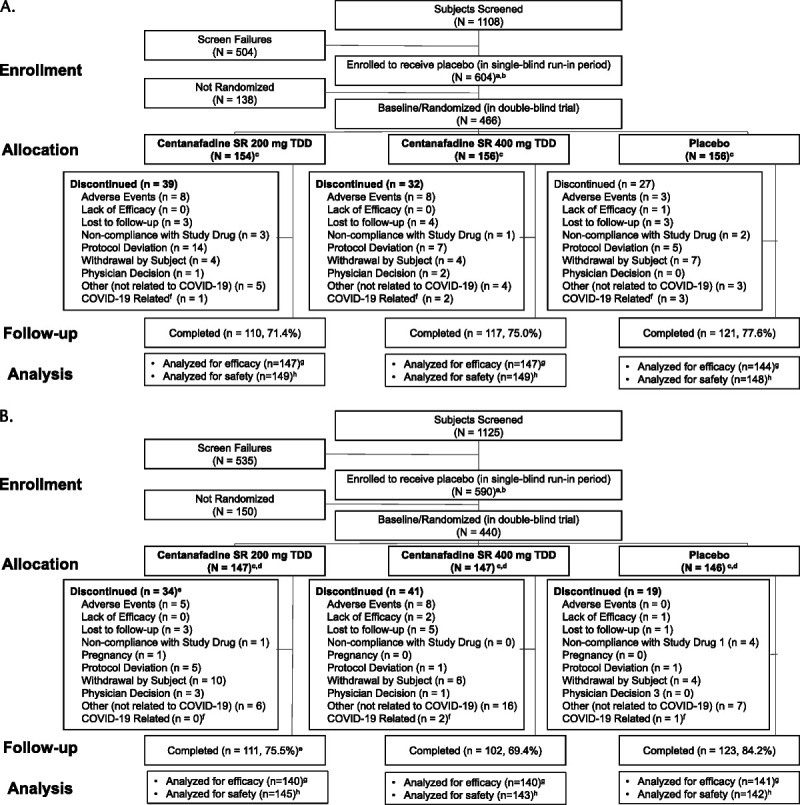
Findings/results: Subjects randomized in study 1 (centanafadine 200 mg/d, n = 149; centanafadine 400 mg/d, n = 149; placebo, n = 148) and study 2 (centanafadine 200 mg/d, n = 145; centanafadine 400 mg/d, n = 143; placebo, n = 142) had moderate to severe ADHD (mean AISRS total score, 38.7 [SD, 6.8] across both studies). At day 42, statistically significant least-squares mean differences in AISRS total score were observed in favor of centanafadine versus placebo in study 1 (200 mg/d: -3.16, P = 0.019; 400 mg/d: -2.74, P = 0.039) and study 2 (200 mg/d: -4.01, P = 0.002; 400 mg/d: -4.47, P = 0.001). Effect sizes versus placebo were -0.28 for 200 mg/d and -0.24 for 400 mg/d in study 1 and -0.37 for 200 mg/d and -0.40 for 400 mg/d in study 2. The overall rate of treatment-emergent adverse events (TEAEs) was low, but there was a small increase in TEAE occurrence with increasing dose. Incidences of serious TEAEs and abuse potential-related AEs were low.
Implications/conclusions: These are the first large-scale studies to demonstrate the efficacy and safety profiles of 200 mg/d and 400 mg/d centanafadine in adults with ADHD.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Figures
References
-
- Alexander L, Farrelly N. Attending to adult ADHD: a review of the neurobiology behind adult ADHD. Ir J Psychol Med. 2018;35:237–244. - PubMed
-
- Sharma A, Couture J. A review of the pathophysiology, etiology, and treatment of attention-deficit hyperactivity disorder (ADHD). Ann Pharmacother. 2014;48:209–225. - PubMed
-
- Solanto MV. Neuropsychopharmacological mechanisms of stimulant drug action in attention-deficit hyperactivity disorder: a review and integration. Behav Brain Res. 1998;94:127–152. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
