

Treatment With Adjuvant Abemaciclib Plus Endocrine Therapy in Patients With High-risk Early Breast Cancer Who Received Neoadjuvant Chemotherapy: A Prespecified Analysis of the monarchE Randomized Clinical Trial
- PMID: 35653145
- PMCID: PMC9164117
- DOI: 10.1001/jamaoncol.2022.1488
Treatment With Adjuvant Abemaciclib Plus Endocrine Therapy in Patients With High-risk Early Breast Cancer Who Received Neoadjuvant Chemotherapy: A Prespecified Analysis of the monarchE Randomized Clinical Trial
Abstract
Importance: Patients selected to receive neoadjuvant chemotherapy (NAC) are usually those at higher risk of relapse, and there is a need to find better therapeutic options for these patients.
Objective: To determine the efficacy and safety outcomes for patients with hormone receptor (HR)-positive, ERBB2 (formerly HER2)-, high-risk early breast cancer enrolled in the randomized clinical trial monarchE who received NAC.
Design, setting, and participants: The monarchE randomized clinical trial was a multicenter, phase 3, open-label study that evaluated adjuvant treatment with abemaciclib plus endocrine therapy (ET) compared with ET alone in patients with HR+, ERBB2-, and node-positive early breast cancer who were at high risk of recurrence. Patients were recruited between July 2017 and August 2019 from 603 sites in 38 countries. This subgroup analysis was performed with primary outcome data, with a cutoff date of July 8, 2020.
Intervention: Enrolled patients were randomized (1:1) to receive standard of care ET for at least 5 years with or without treatment with abemaciclib (150 mg, twice daily) for 2 years (treatment period) or until criteria were met for discontinuation.
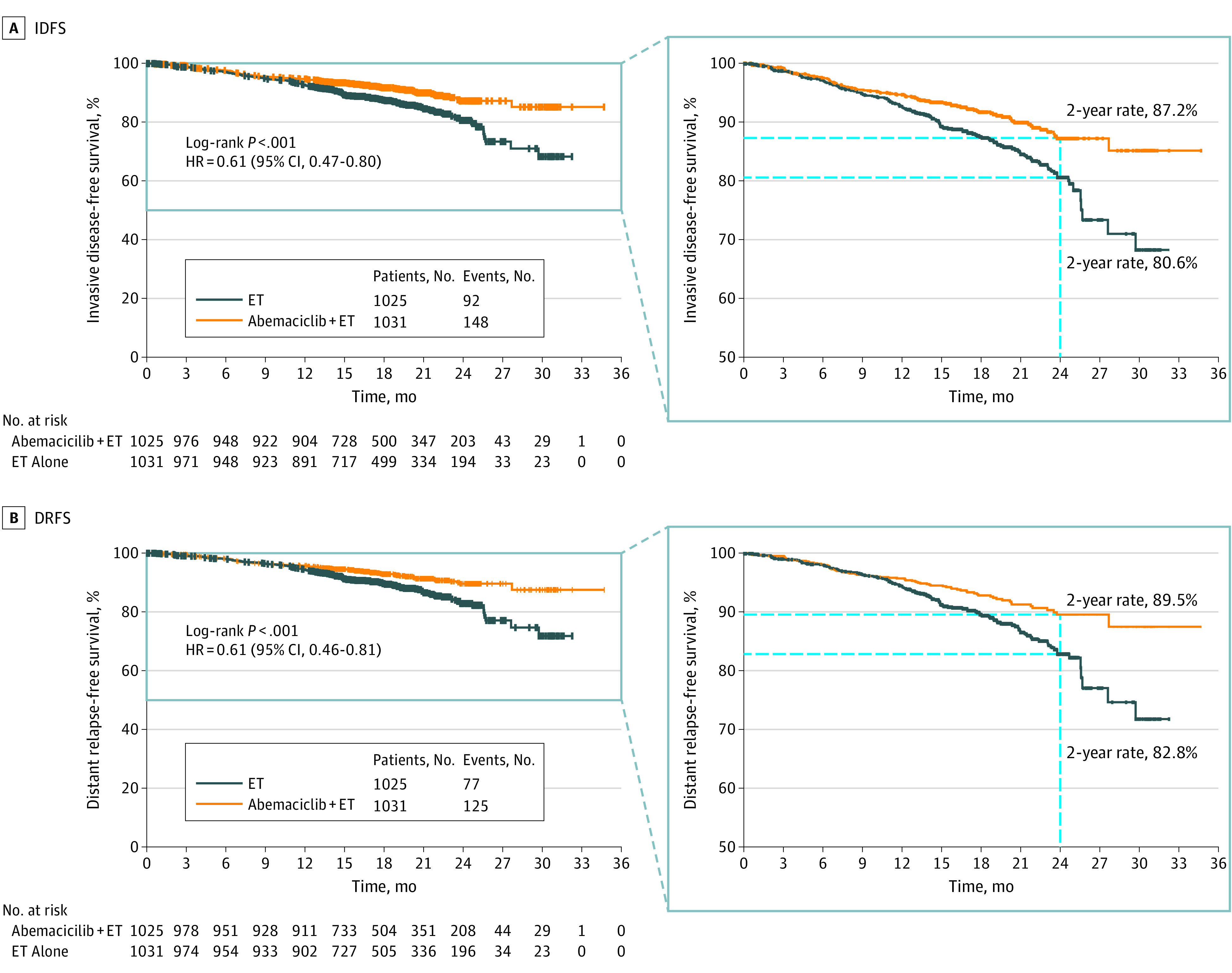
Main outcomes and measures: Prior chemotherapy (NAC vs adjuvant vs none) was a stratification factor in monarchE, and and a prespecified exploratory analysis included outcomes in patients who received NAC. The data presented in this article are from the primary outcome analysis (395 invasive disease-free survival [IDFS] events; cutoff date, July 8, 2020; median follow-up 19 months [IQR, 15.6-23.9 months]). Invasive disease-free survival (the primary end point of monarchE) and distant relapse-free survival (DRFS) were evaluated using the Cox proportional hazard model and Kaplan-Meier method.
Results: Of the 5637 patients (mean [SD] age, 49.9 [10.6] years; 2046 women [99.5%]; 462 Asian [22.8%], 54 Black [2.7%], and 1473 White participants [70.8%]) enrolled in monarchE, 2056 (37%) received treatment with NAC. In this subgroup, treatment with abemaciclib and ET demonstrated clinically meaningful benefit in IDFS (hazard ratio, 0.61; 95% CI, 0.47-0.80) and DRFS (hazard ratio, 0.61; 95% CI, 0.46-0.81), which corresponded with an absolute improvement of 6.6% in 2-year IDFS rates and 6.7% in 2-year DRFS rates. A consistent treatment benefit was observed across subgroups of pathological breast tumor size or number of positive lymph nodes at surgery.
Conclusions and relevance: In the randomized clinical trial monarchE, treatment with adjuvant abemaciclib combined with ET demonstrated a clinically meaningful improvement in IDFS and DRFS for patients with HR+, ERBB2-, node-positive, high-risk early breast cancer who received NAC before trial enrollment.
Trial registration: ClinicalTrials.gov Identifier: NCT03155997.
Conflict of interest statement
Figures
Comment in
-
Quantifying Clinical Utility of Adjuvant Abemaciclib in Patients With High-risk Early Breast Cancer Who Received Neoadjuvant Chemotherapy.JAMA Oncol. 2022 Nov 1;8(11):1701. doi: 10.1001/jamaoncol.2022.4528. JAMA Oncol. 2022. PMID: 36173642 No abstract available.
References
-
- National Comprehensive Cancer Network . NCCN clinical practice guidelines in oncology: breast cancer, version 5.2020. Accessed September 3, 2021. https://www2.tri-kobe.org/nccn/guideline/breast/english/breast.pdf - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
