

Prospective Studies Comparing Structured vs Nonstructured Diagnostic Protocol Evaluations Among Patients With Fever of Unknown Origin: A Systematic Review and Meta-analysis
- PMID: 35653154
- PMCID: PMC9164007
- DOI: 10.1001/jamanetworkopen.2022.15000
Prospective Studies Comparing Structured vs Nonstructured Diagnostic Protocol Evaluations Among Patients With Fever of Unknown Origin: A Systematic Review and Meta-analysis
Abstract
Importance: Patients meeting the criteria for fever of unknown origin (FUO) can be evaluated with structured or nonstructured approaches, but the optimal diagnostic method is unresolved.
Objective: To analyze differences in diagnostic outcomes among patients undergoing structured or nonstructured diagnostic methods applied to prospective clinical studies.
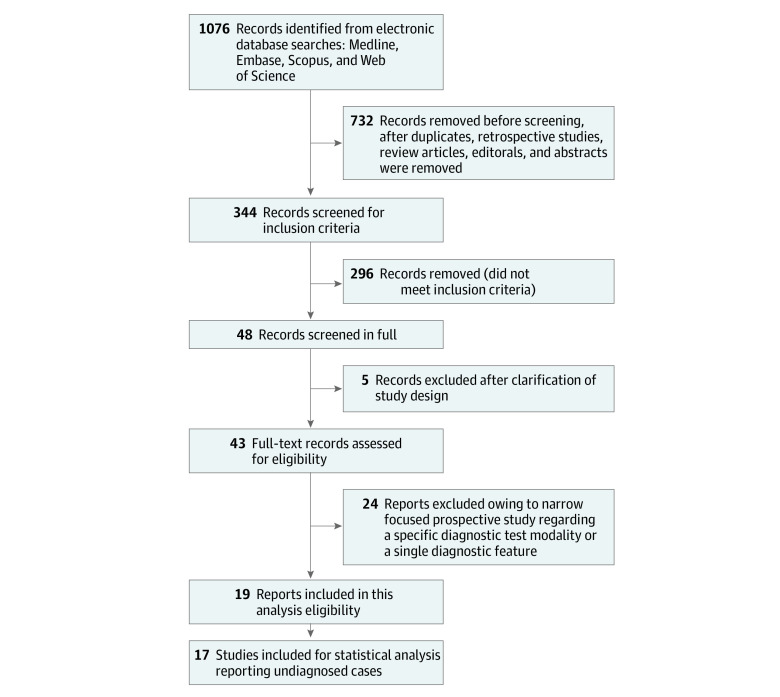
Data sources: PubMed, Embase, Scopus, and Web of Science databases with librarian-generated query strings for FUO, PUO, fever or pyrexia of unknown origin, clinical trial, and prospective studies identified from January 1, 1997, to March 31, 2021.
Study selection: Prospective studies meeting any adult FUO definition were included. Articles were excluded if patients did not precisely fit any existing adult FUO definition or studies were not classified as prospective.
Data extraction and synthesis: Abstracted data included years of publication and study period, country, setting (eg, university vs community hospital), defining criteria and category outcome, structured or nonstructured diagnostic protocol evaluation, sex, temperature threshold and measurement, duration of fever and hospitalization before final diagnoses, and contribution of potential diagnostic clues, biochemical and immunological serologic studies, microbiology cultures, histologic analysis, and imaging studies. Structured protocols compared with nonstructured diagnostic methods were analyzed using regression models.
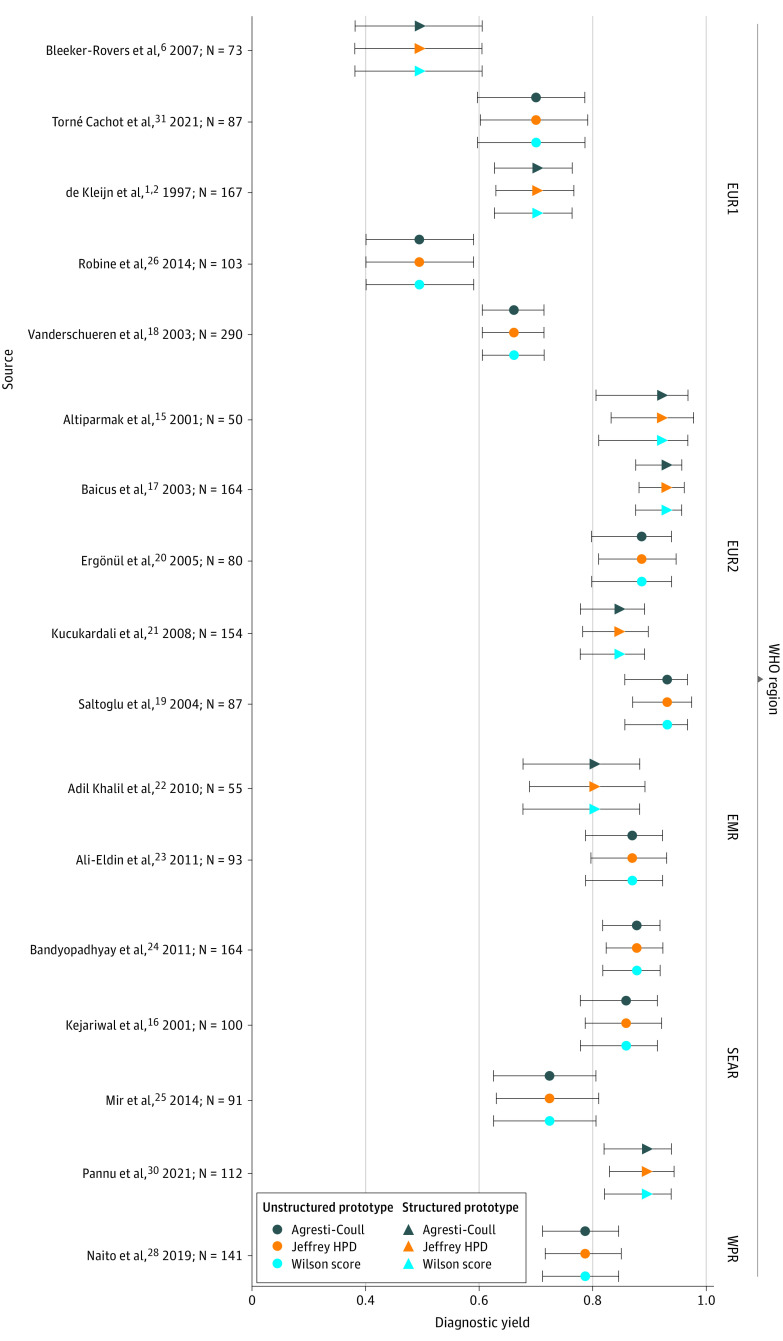
Main outcomes and measures: Overall diagnostic yield was the primary outcome.
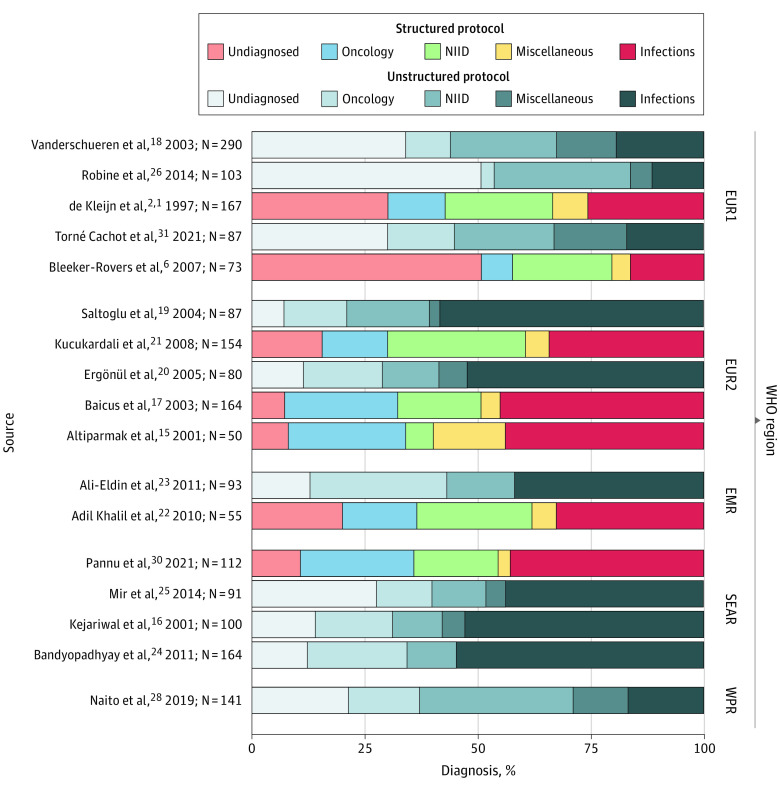
Results: Among the 19 prospective trials with 2627 unique patients included in the analysis (range of patient ages, 10-94 years; 21.0%-55.3% female), diagnoses among FUO series varied across and within World Health Organization (WHO) geographic regions. Use of a structured diagnostic protocol was not significantly associated with higher odds of yielding a diagnosis compared with nonstructured protocols in aggregate (odds ratio [OR], 0.98; 95% CI, 0.65-1.49) or between Western Europe (Belgium, France, the Netherlands, and Spain) (OR, 0.95; 95% CI, 0.49-1.86) and Eastern Europe (Turkey and Romania) (OR, 0.83; 95% CI, 0.41-1.69). Despite the limited number of studies in some regions, analyses based on the 6 WHO geographic areas found differences in the diagnostic yield. Western European studies had the lowest percentage of achieving a diagnosis. Southeast Asia led with infections at 49.0%. Noninfectious inflammatory conditions were most prevalent in the Western Pacific region (34.0%), whereas the Eastern Mediterranean region had the highest proportion of oncologic explanations (24.0%).
Conclusions and relevance: In this systematic review and meta-analysis, diagnostic yield varied among WHO regions. Available evidence from prospective studies did not support that structured diagnostic protocols had a significantly better rate of achieving a diagnosis than nonstructured protocols. Clinicians worldwide should incorporate geographical disease prevalence in their evaluation of patients with FUO.
Conflict of interest statement
Figures
References
-
- de Kleijn EM, Vandenbroucke JP, van der Meer JW; The Netherlands FUO Study Group . Fever of unknown origin (FUO), I: a prospective multicenter study of 167 patients with FUO, using fixed epidemiologic entry criteria. Medicine (Baltimore). 1997;76(6):392-400. doi:10.1097/00005792-199711000-00002 - DOI - PubMed
-
- Durack DT, Street AC. Fever of unknown origin—reexamined and redefined. Curr Clin Top Infect Dis. 1991;11:35-51. - PubMed
