Prognostic indicators and outcomes of hospitalised COVID-19 patients with neurological disease: An individual patient data meta-analysis
- PMID: 35653330
- PMCID: PMC9162376
- DOI: 10.1371/journal.pone.0263595
Prognostic indicators and outcomes of hospitalised COVID-19 patients with neurological disease: An individual patient data meta-analysis
Abstract
Background: Neurological COVID-19 disease has been reported widely, but published studies often lack information on neurological outcomes and prognostic risk factors. We aimed to describe the spectrum of neurological disease in hospitalised COVID-19 patients; characterise clinical outcomes; and investigate factors associated with a poor outcome.
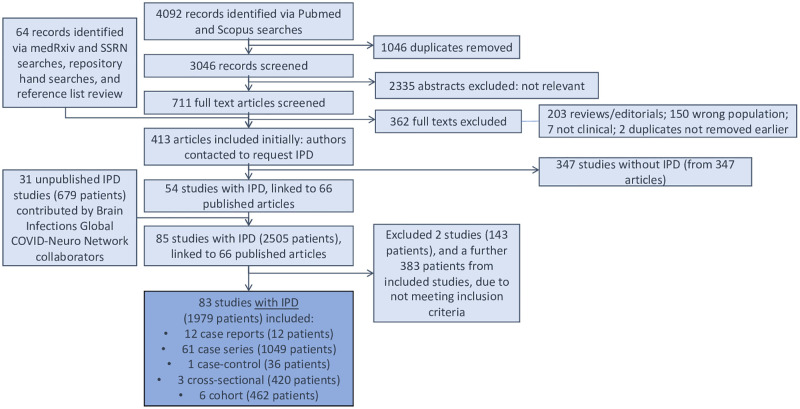
Methods: We conducted an individual patient data (IPD) meta-analysis of hospitalised patients with neurological COVID-19 disease, using standard case definitions. We invited authors of studies from the first pandemic wave, plus clinicians in the Global COVID-Neuro Network with unpublished data, to contribute. We analysed features associated with poor outcome (moderate to severe disability or death, 3 to 6 on the modified Rankin Scale) using multivariable models.
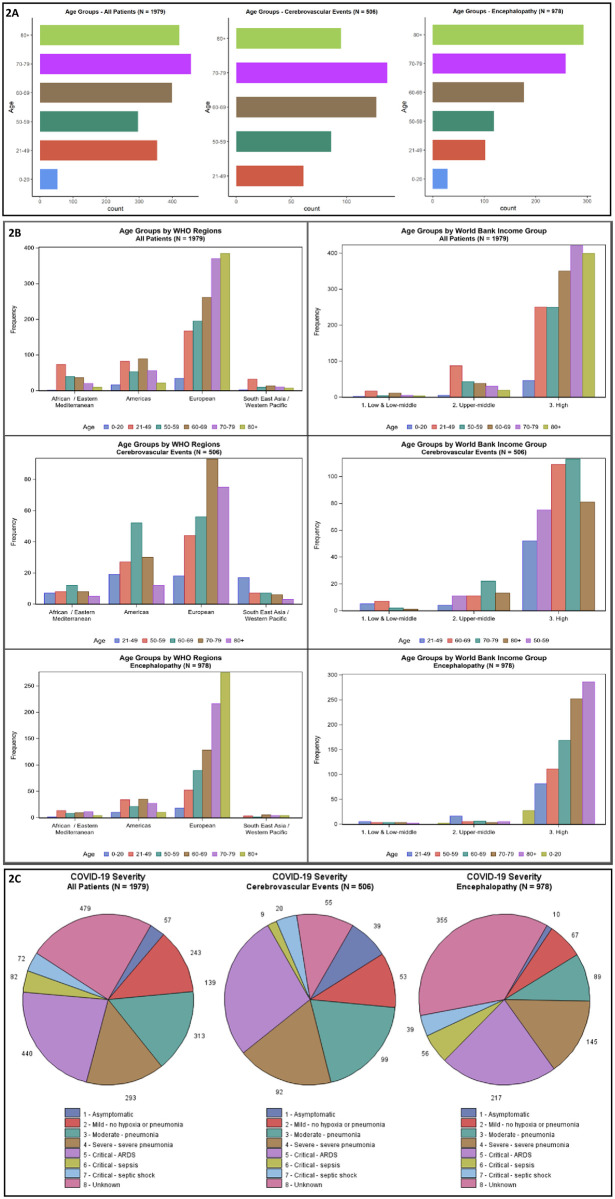
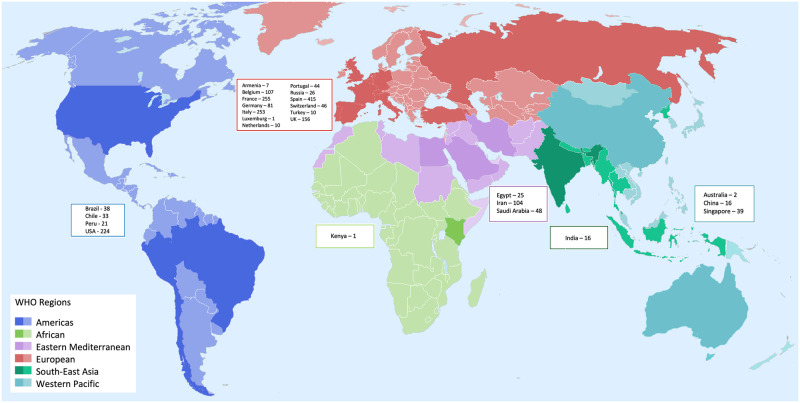
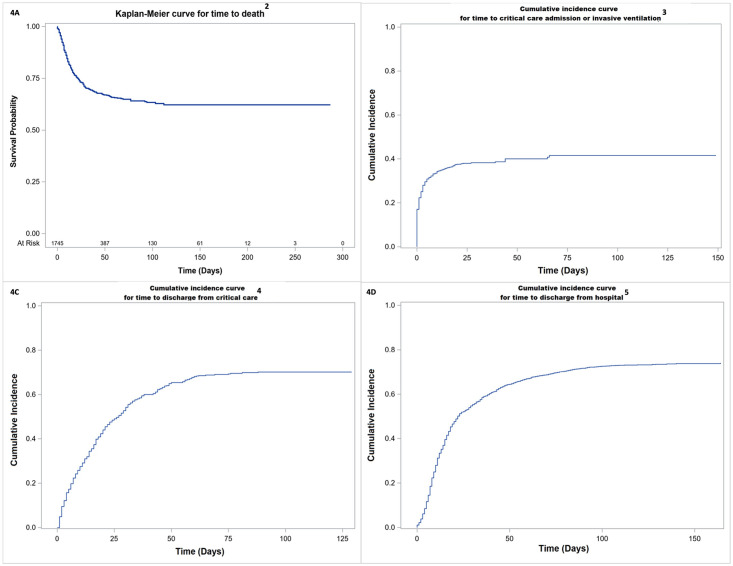
Results: We included 83 studies (31 unpublished) providing IPD for 1979 patients with COVID-19 and acute new-onset neurological disease. Encephalopathy (978 [49%] patients) and cerebrovascular events (506 [26%]) were the most common diagnoses. Respiratory and systemic symptoms preceded neurological features in 93% of patients; one third developed neurological disease after hospital admission. A poor outcome was more common in patients with cerebrovascular events (76% [95% CI 67-82]), than encephalopathy (54% [42-65]). Intensive care use was high (38% [35-41]) overall, and also greater in the cerebrovascular patients. In the cerebrovascular, but not encephalopathic patients, risk factors for poor outcome included breathlessness on admission and elevated D-dimer. Overall, 30-day mortality was 30% [27-32]. The hazard of death was comparatively lower for patients in the WHO European region.
Interpretation: Neurological COVID-19 disease poses a considerable burden in terms of disease outcomes and use of hospital resources from prolonged intensive care and inpatient admission; preliminary data suggest these may differ according to WHO regions and country income levels. The different risk factors for encephalopathy and stroke suggest different disease mechanisms which may be amenable to intervention, especially in those who develop neurological symptoms after hospital admission.
Conflict of interest statement
TS is part of the Data Safety Monitoring Committee of a study to evaluate the safety and immunogenicity of a candidate Ebola Vaccine in children - the GSK3390107A (ChAd3 EBO-Z) vaccine; he is a panel member of Covid-19 Vaccine Benefit Risk Expert Working Group for the Medicines and Healthcare Regulatory Agency (UK); he is a member of COVID-19 Therapeutics Advisory Panel for the UK Department of Health & Social Care; he is the Chair/Co-Chair of the COVID-19 Rapid Response and Rolling Funding Initiatives, which supported the development of the Oxford-AstraZeneca Covid-19 vaccine. In addition, Dr. Solomon has a diagnostic test for bacterial meningitis, based on a blood test, filed for patent pending.
Figures