

A multi-population phenome-wide association study of genetically-predicted height in the Million Veteran Program
- PMID: 35653334
- PMCID: PMC9162317
- DOI: 10.1371/journal.pgen.1010193
A multi-population phenome-wide association study of genetically-predicted height in the Million Veteran Program
Abstract
Background: Height has been associated with many clinical traits but whether such associations are causal versus secondary to confounding remains unclear in many cases. To systematically examine this question, we performed a Mendelian Randomization-Phenome-wide association study (MR-PheWAS) using clinical and genetic data from a national healthcare system biobank.
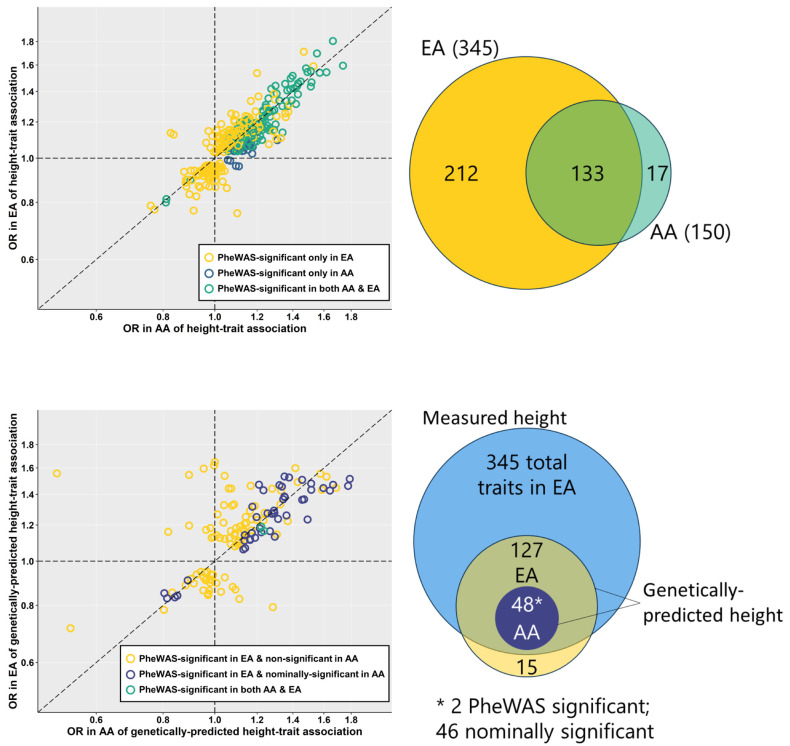
Methods and findings: Analyses were performed using data from the US Veterans Affairs (VA) Million Veteran Program in non-Hispanic White (EA, n = 222,300) and non-Hispanic Black (AA, n = 58,151) adults in the US. We estimated height genetic risk based on 3290 height-associated variants from a recent European-ancestry genome-wide meta-analysis. We compared associations of measured and genetically-predicted height with phenome-wide traits derived from the VA electronic health record, adjusting for age, sex, and genetic principal components. We found 345 clinical traits associated with measured height in EA and an additional 17 in AA. Of these, 127 were associated with genetically-predicted height at phenome-wide significance in EA and 2 in AA. These associations were largely independent from body mass index. We confirmed several previously described MR associations between height and cardiovascular disease traits such as hypertension, hyperlipidemia, coronary heart disease (CHD), and atrial fibrillation, and further uncovered MR associations with venous circulatory disorders and peripheral neuropathy in the presence and absence of diabetes. As a number of traits associated with genetically-predicted height frequently co-occur with CHD, we evaluated effect modification by CHD status of genetically-predicted height associations with risk factors for and complications of CHD. We found modification of effects of MR associations by CHD status for atrial fibrillation/flutter but not for hypertension, hyperlipidemia, or venous circulatory disorders.
Conclusions: We conclude that height may be an unrecognized but biologically plausible risk factor for several common conditions in adults. However, more studies are needed to reliably exclude horizontal pleiotropy as a driving force behind at least some of the MR associations observed in this study.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: CJO is a full-time employee of Novartis Institutes of Biomedical Research. The remaining authors have declared that no competing interests exist.
Figures



References
Publication types
MeSH terms
Grants and funding
- UM1 DK126194/DK/NIDDK NIH HHS/United States
- R01 HL143885/HL/NHLBI NIH HHS/United States
- R01 HL142302/HL/NHLBI NIH HHS/United States
- R01 DK101478/DK/NIDDK NIH HHS/United States
- I01 BX003362/BX/BLRD VA/United States
- R01 HG010297/HG/NHGRI NIH HHS/United States
- R01 DK122503/DK/NIDDK NIH HHS/United States
- R56 DK101478/DK/NIDDK NIH HHS/United States
- I01 BX004821/BX/BLRD VA/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- R01 HG009974/HG/NHGRI NIH HHS/United States
- R01 DK101855/DK/NIDDK NIH HHS/United States
- IK2 CX001907/CX/CSRD VA/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
