

SARS-CoV-2 Omicron variant escapes neutralizing antibodies and T cell responses more efficiently than other variants in mild COVID-19 convalescents
- PMID: 35654046
- PMCID: PMC9110310
- DOI: 10.1016/j.xcrm.2022.100651
SARS-CoV-2 Omicron variant escapes neutralizing antibodies and T cell responses more efficiently than other variants in mild COVID-19 convalescents
Abstract
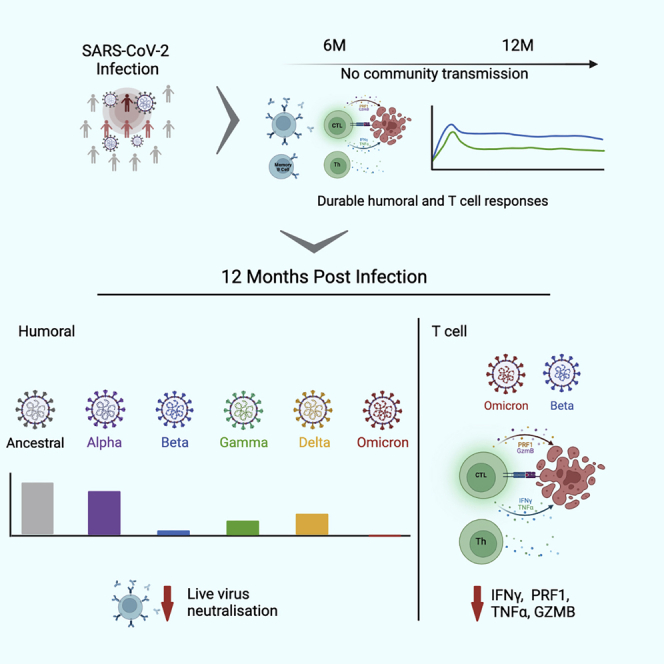
Coronavirus disease 2019 (COVID-19) convalescents living in regions with low vaccination rates rely on post-infection immunity for protection against re-infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). We evaluate humoral and T cell immunity against five variants of concern (VOCs) in mild-COVID-19 convalescents at 12 months after infection with ancestral virus. In this cohort, ancestral, receptor-binding domain (RBD)-specific antibody and circulating memory B cell levels are conserved in most individuals, and yet serum neutralization against live B.1.1.529 (Omicron) is completely abrogated and significantly reduced for other VOCs. Likewise, ancestral SARS-CoV-2-specific memory T cell frequencies are maintained in >50% of convalescents, but the cytokine response in these cells to mutated spike epitopes corresponding to B.1.1.529 and B.1.351 (Beta) VOCs were impaired. These results indicate that increased antigen variability in VOCs impairs humoral and spike-specific T cell immunity post-infection, strongly suggesting that COVID-19 convalescents are vulnerable and at risk of re-infection with VOCs, thus stressing the importance of vaccination programs.
Keywords: SARS-CoV-2; T cell immunity; Variant of Concern; antibody response; antigen drift; memory B cells; virus neutralization.
Copyright © 2022 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests A.S. is currently a consultant for Gritstone, Flow Pharma, Arcturus, Epitogenesis, Oxfordimmunotech, Caprion, and Avalia. La Jolla Institute for Immunology (A.S. and D.W.) has filed for patent protection for various aspects of T cell epitope and vaccine design work. P.G.-V., C.M.H., M.G.M., A.E.L.Y., H.B., Z.A.M., Z.A.-D., A. Abayasingam, D.A., A.O.S., A. Aggarwal, G.B., J.G., C.F., S.O., E.M.M., D.J.L., G.M., E.J.G., B.A.J.R., D.S., C.K.-L., S.G.T., M.R.B., D.W., R.A.B., S.C.B., and B.G.-B. declare no conflicts of interest.
Figures







References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
