

Functional Outcome after Spinal Meningioma Surgery
- PMID: 35654108
- PMCID: PMC9633248
- DOI: 10.31616/asj.2021.0201
Functional Outcome after Spinal Meningioma Surgery
Abstract
Study design: A multicenter cross-sectional analytical retrospective study.
Purpose: To assess functional outcome (FO) after a spinal meningioma (SM) surgery.
Overview of literature: All studies report functional improvement after SM removal.
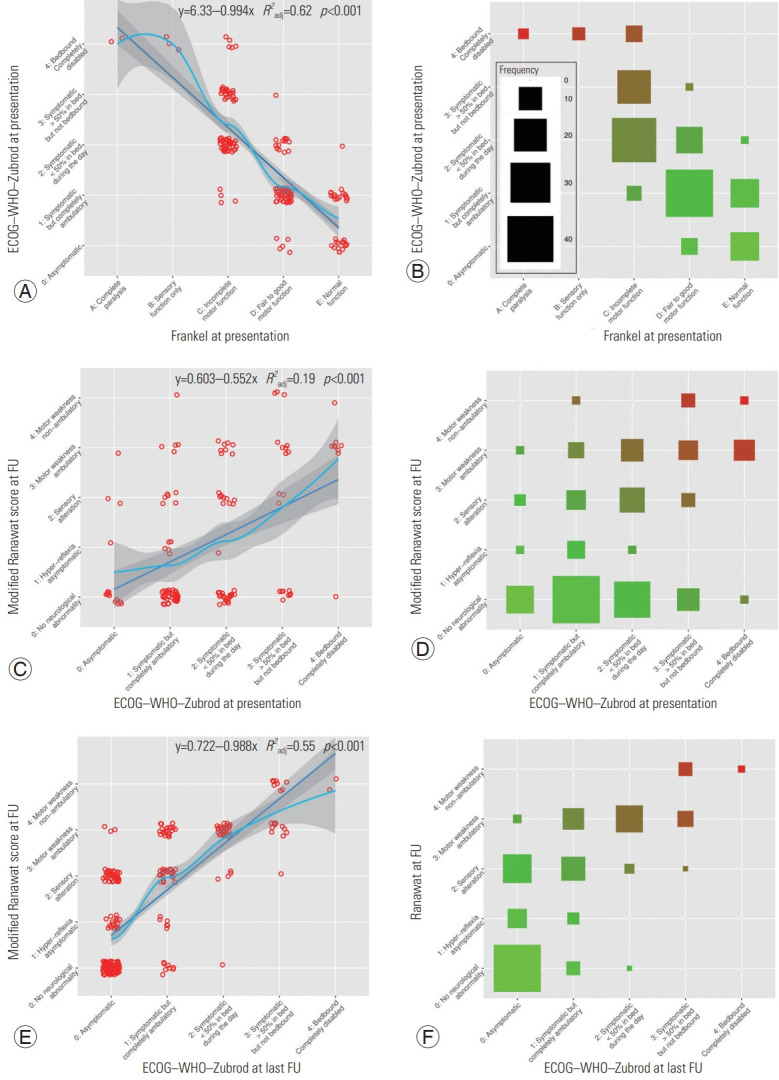
Methods: We performed an analytical retrospective cohort study at five different institutions. All patients with a diagnosis of SM were included in this study, including those with recurrent tumors. Meningiomas of the foramen magnum were excluded. Useful histopathological characteristics were separately extracted. Surgical resection was evaluated according to the Simpson grading scale. Patient outcomes and clinical states were assessed with the help of their medical records using four different scales: the modified Ranawat score, the Nurick scale, the Prolo score, the Frankel grade, and the Eastern Cooperative Oncology Group-World Health Organization- Zubrod score.
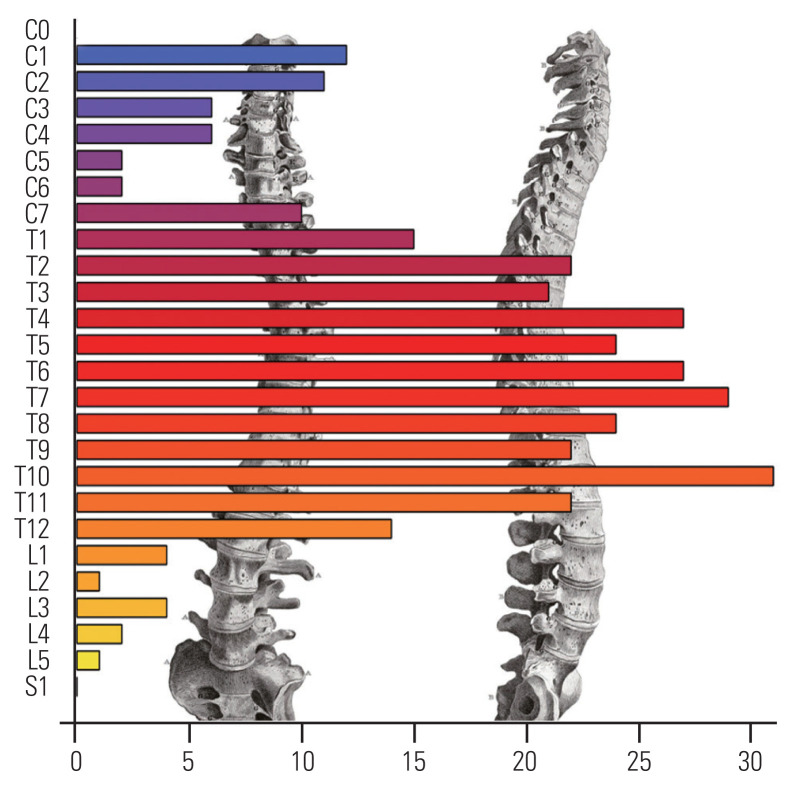
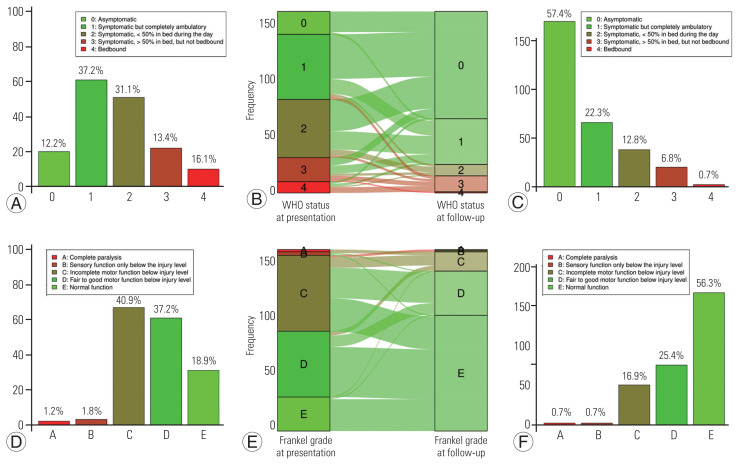
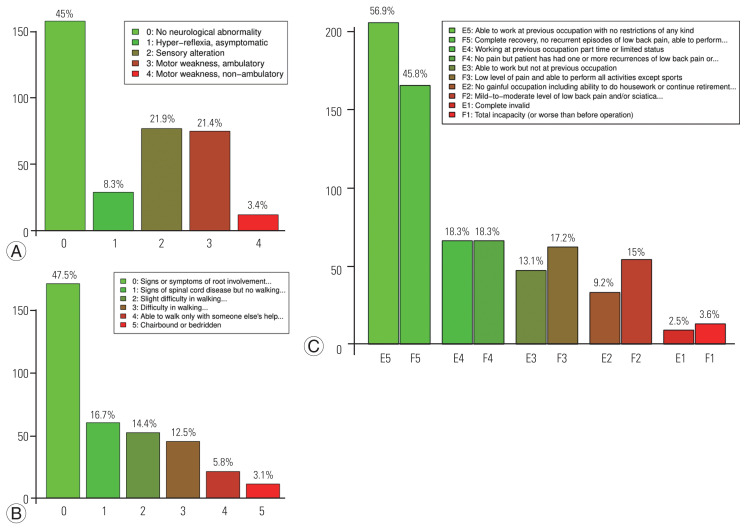
Results: Between 1991 and 2018, 417 patients were identified, of which 85.8% were female. The median age at surgery was 67.2 years (interquartile range [IQR], 56.7-76.5). The lesion was located in the thoracic region in 77.9% of the patients, cervical region in 16.8%, and lumbar region in 4.1%. Surgical resection was complete in 95.5% of the cases. Only 0.96% of the patients died within the first postoperative month. Neurological status, which improved in 76.9% of the patients, was unchanged in 17.5% and even worsened in 4.4%. Functional status was assessed using the Ranawat score and Nurick scale, with scores of 1 (IQR, 0-2) (i.e., hyperreflexia and asymptomatic; mean, 1.3±1.3) and 1 (IQR, 0-2) (i.e., signs of spinal cord disease, but no difficulty in walking; mean, 1.2±1.4), respectively. Approximately 10.1% of the patients were not ambulant at the last neurosurgical follow-up visit. Older age at surgery was not significantly associated with a chair-bound status (p =0.427).
Conclusions: This large series confirms the favorable FO after spinal meningioma surgery even in the case of seriously impaired preoperative status. A validated scale is needed to assess the factors predicting a worsening of the functional status and guide the management of patients.
Keywords: Functional outcome; Meningioma; Spine.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Champeaux C, Weller J, Katsahian S. Epidemiology of meningiomas: a nationwide study of surgically treated tumours on French medico-administrative data. Cancer Epidemiol. 2019;58:63–70. - PubMed
-
- Zouaoui S, Darlix A, Rigau V, et al. Descriptive epidemiology of 13,038 newly diagnosed and histologically confirmed meningiomas in France: 2006–2010. Neurochirurgie. 2018;64:15–21. - PubMed
-
- Champeaux-Depond C, Weller J, Resche-Rigon M. Neurofibromatosis type 2: a nationwide population-based study focused on survival after meningioma surgery. Clin Neurol Neurosurg. 2020;198:106236. - PubMed
-
- Champeaux-Depond C, Weller J, Froelich S, Sartor A. Cyproterone acetate and meningioma: a nationwide-wide population based study. J Neurooncol. 2021;151:331–8. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
