

Episodic Ataxia Type 1: Natural History and Effect on Quality of Life
- PMID: 35655106
- PMCID: PMC10307716
- DOI: 10.1007/s12311-021-01360-6
Episodic Ataxia Type 1: Natural History and Effect on Quality of Life
Erratum in
-
Correction to: Episodic Ataxia Type 1: Natural History and Effect on Quality of Life.Cerebellum. 2023 Aug;22(4):587. doi: 10.1007/s12311-022-01450-z. Cerebellum. 2023. PMID: 35904745 Free PMC article. No abstract available.
Abstract
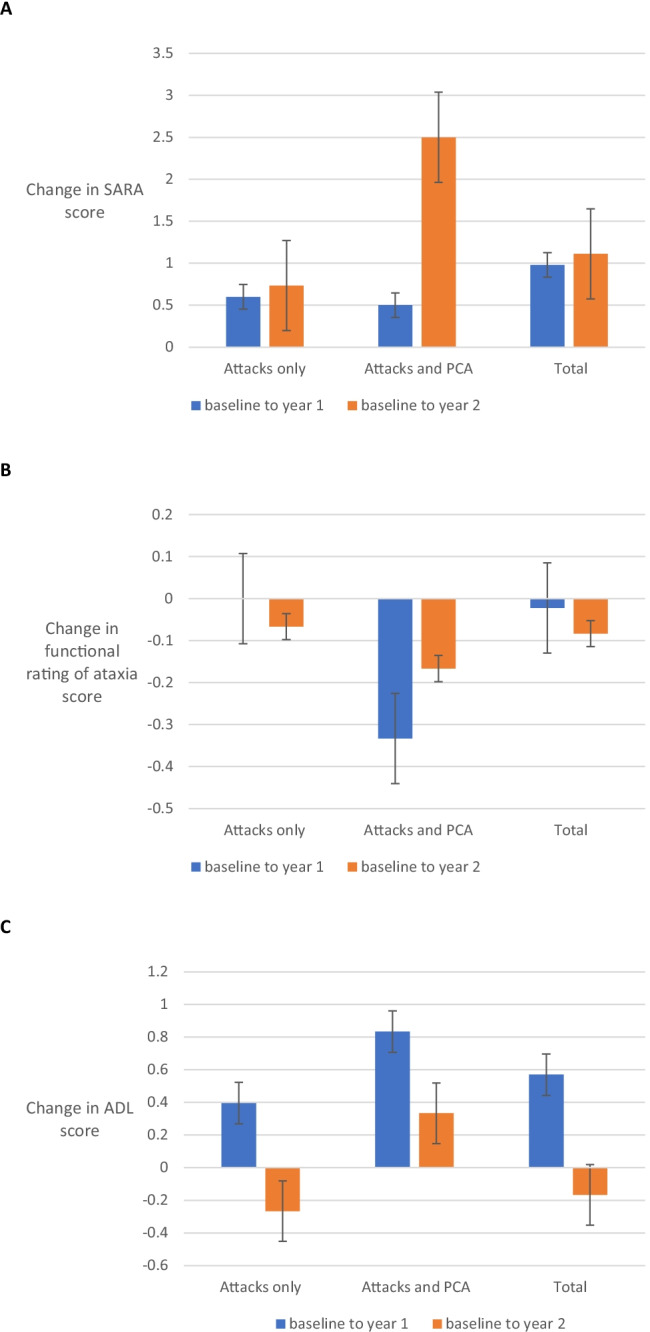
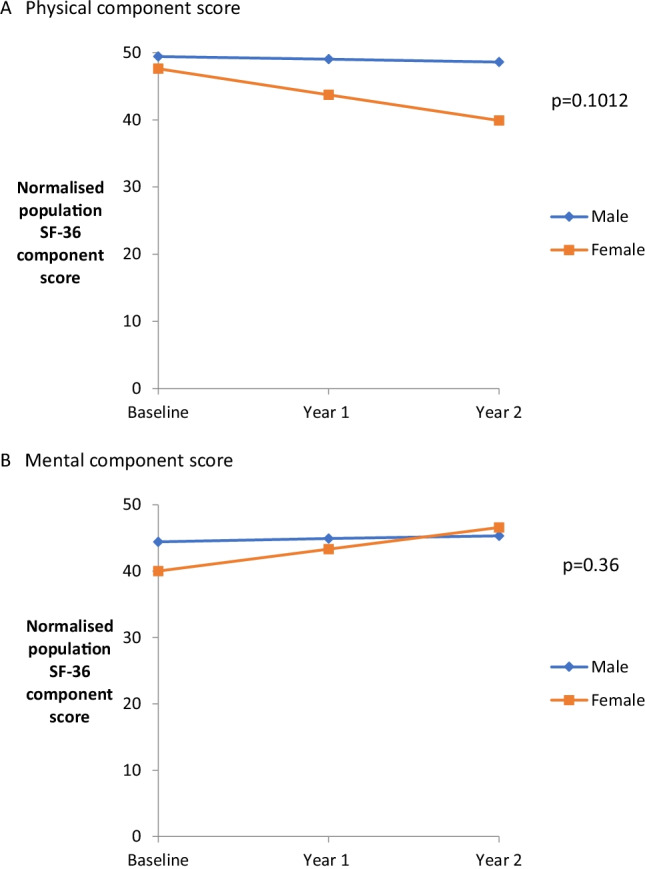
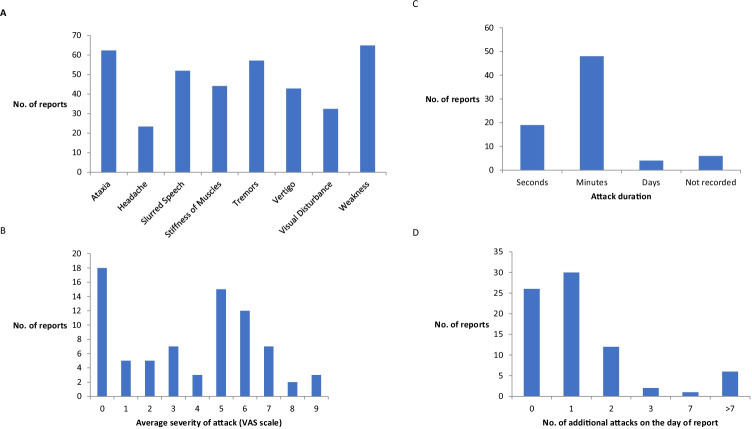
Episodic ataxia type 1 (EA1) is a rare autosomal potassium channelopathy, due to mutations in KCNA1. Patients have childhood onset of intermittent attacks of ataxia, dizziness or imbalance. In order to quantify the natural history of EA1, its effect on quality of life and in preparation for future clinical trials, we set up an international multi-centre study of EA1. We recruited thirty-three participants with EA1: twenty-three completed 1-year follow-up and eighteen completed 2-year follow-up. There was very little accumulation of disability or impairment over the course of the 2 years of the study. The outcome measures of ataxia (SARA and functional rating of ataxia) and the activities of daily living scale were largely stable over time. Self-reported health-related quality of life (SF-36) scores were lower across all domains than controls, in keeping with a chronic condition. Physical subdomain scores appeared to deteriorate over time, which seems to be driven by the female participants in the study. This is an interesting finding and warrants further study. Attacks of EA1 reported by participants in real time via an interactive voice response system showed that symptoms were not stereotyped; however, attack duration and frequency was stable between individuals. This large prospective study is the first ever completed in subjects with EA1. We document the natural history of the disorder over 2 years. These data will enable the development of outcome measures for clinical trials of treatment.
Keywords: EA1; Episodic ataxia type 1; KCNA1; Natural history; SF-36.
© 2022. Crown.
Conflict of interest statement
• The authors have no relevant financial or non-financial interests to disclose.
• The authors have no conflicts of interest to declare that are relevant to the content of this article.
• All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Figures

References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
