Prognostic implications of comorbidity patterns in critically ill COVID-19 patients: A multicenter, observational study
- PMID: 35655660
- PMCID: PMC9148543
- DOI: 10.1016/j.lanepe.2022.100422
Prognostic implications of comorbidity patterns in critically ill COVID-19 patients: A multicenter, observational study
Abstract
Background: The clinical heterogeneity of COVID-19 suggests the existence of different phenotypes with prognostic implications. We aimed to analyze comorbidity patterns in critically ill COVID-19 patients and assess their impact on in-hospital outcomes, response to treatment and sequelae.
Methods: Multicenter prospective/retrospective observational study in intensive care units of 55 Spanish hospitals. 5866 PCR-confirmed COVID-19 patients had comorbidities recorded at hospital admission; clinical and biological parameters, in-hospital procedures and complications throughout the stay; and, clinical complications, persistent symptoms and sequelae at 3 and 6 months.
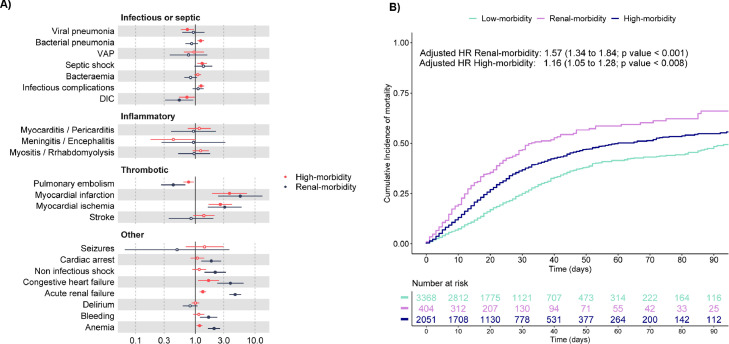
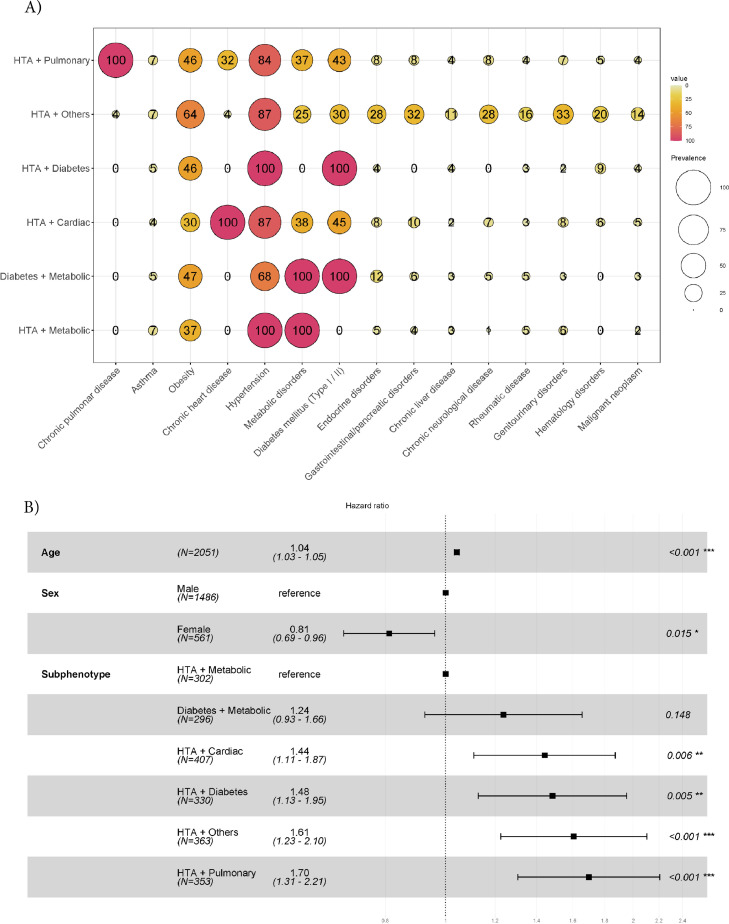
Findings: Latent class analysis identified 3 phenotypes using training and test subcohorts: low-morbidity (n=3385; 58%), younger and with few comorbidities; high-morbidity (n=2074; 35%), with high comorbid burden; and renal-morbidity (n=407; 7%), with chronic kidney disease (CKD), high comorbidity burden and the worst oxygenation profile. Renal-morbidity and high-morbidity had more in-hospital complications and higher mortality risk than low-morbidity (adjusted HR (95% CI): 1.57 (1.34-1.84) and 1.16 (1.05-1.28), respectively). Corticosteroids, but not tocilizumab, were associated with lower mortality risk (HR (95% CI) 0.76 (0.63-0.93)), especially in renal-morbidity and high-morbidity. Renal-morbidity and high-morbidity showed the worst lung function throughout the follow-up, with renal-morbidity having the highest risk of infectious complications (6%), emergency visits (29%) or hospital readmissions (14%) at 6 months (p<0.01).
Interpretation: Comorbidity-based phenotypes were identified and associated with different expression of in-hospital complications, mortality, treatment response, and sequelae, with CKD playing a major role. This could help clinicians in day-to-day decision making including the management of post-discharge COVID-19 sequelae.
Funding: ISCIII, UNESPA, CIBERES, FEDER, ESF.
Keywords: COVID-19; Critical Care; Prognosis.
© 2022 The Author(s).
Conflict of interest statement
None declared.
Figures