

Vascular Calcification in Chronic Kidney Disease: An Update and Perspective
- PMID: 35656113
- PMCID: PMC9116919
- DOI: 10.14336/AD.2021.1024
Vascular Calcification in Chronic Kidney Disease: An Update and Perspective
Abstract
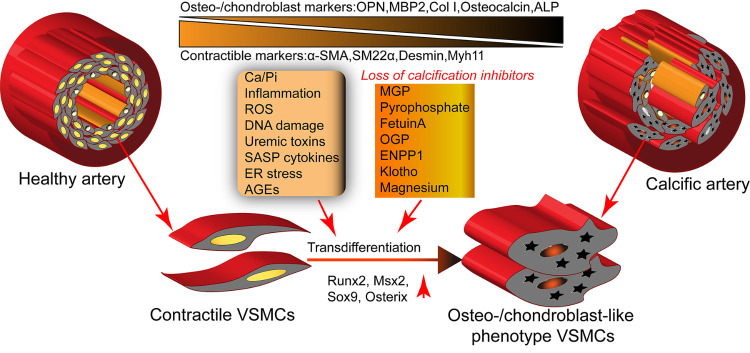
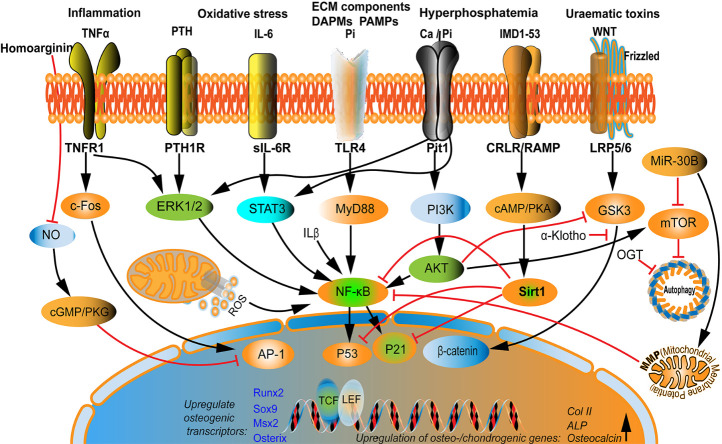
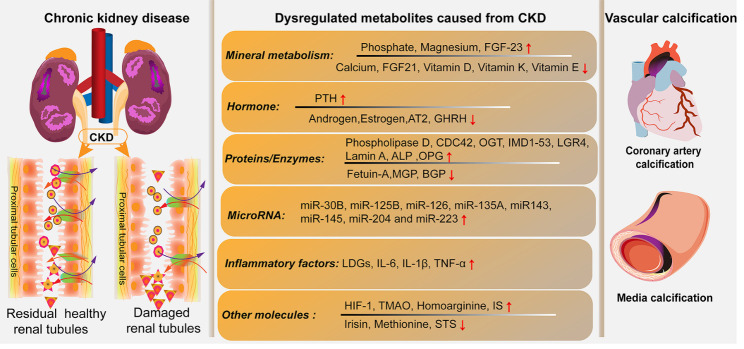
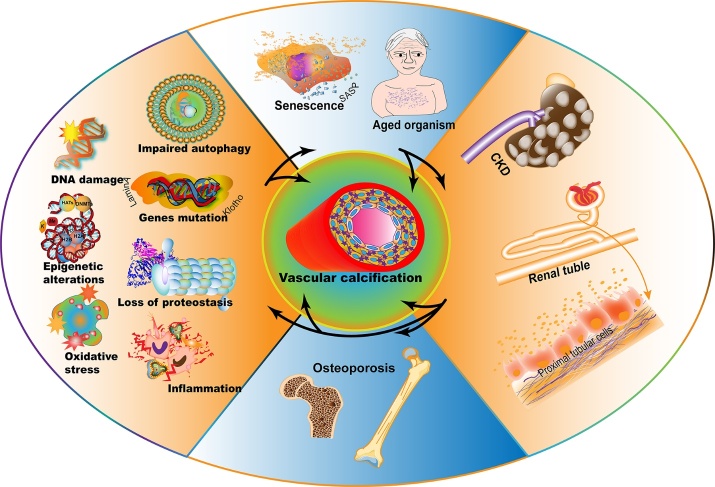
Chronic kidney disease is a devastating condition resulting from irreversible loss of nephron numbers and function and leading to end-stage renal disease and mineral disorders. Vascular calcification, an ectopic deposition of calcium-phosphate salts in blood vessel walls and heart valves, is an independent risk factor of cardiovascular morbidity and mortality in chronic kidney disease. Moreover, aging and related metabolic disorders are essential risk factors for chronic kidney disease and vascular calcification. Marked progress has been recently made in understanding and treating vascular calcification in chronic kidney disease. However, there is a paucity of systematic reviews summarizing this progress, and investigating unresolved issues is warranted. In this systematic review, we aimed to overview the underlying mechanisms of vascular calcification in chronic kidney diseases and discuss the impact of chronic kidney disease on the pathophysiology of vascular calcification. Additionally, we summarized potential clinical diagnostic biomarkers and therapeutic applications for vascular calcification with chronic kidney disease. This review may offer new insights into the pathogenesis, diagnosis, and therapeutic intervention of vascular calcification.
Keywords: aging; biomarker; chronic kidney disease; metabolism; vascular calcification.
Copyright: © 2022 Ren et al.
Conflict of interest statement
Conflicts of interest All authors declare that there are no conflicts of interest or competing interests.
Figures
References
-
- Pescatore LA, Gamarra LF, Liberman M (2019). Multifaceted Mechanisms of Vascular Calcification in Aging. Arterioscler Thromb Vasc Biol, 39:1307-1316. - PubMed
-
- Raggi P (2017). Cardiovascular disease: Coronary artery calcification predicts risk of CVD in patients with CKD. Nat Rev Nephrol, 13:324-326. - PubMed
-
- Tuersun T, Luo Q, Zhang Z, Wang G, Zhang D, Wang M, et al. (2020). Abdominal aortic calcification is more severe in unilateral primary aldosteronism patients and is associated with elevated aldosterone and parathyroid hormone levels. Hypertens Res, 43:1413-1420. - PubMed
LinkOut - more resources
Full Text Sources