

doi: 10.4244/EIJ-D-21-01034.
Management of in-stent restenosis
Affiliations
- PMID: 35656726
- PMCID: PMC9904384
- DOI: 10.4244/EIJ-D-21-01034
Item in Clipboard
Management of in-stent restenosis
EuroIntervention.
.
Abstract
In-stent restenosis (ISR) remains the most common cause of stent failure after percutaneous coronary intervention (PCI). Recent data suggest that ISR-PCI accounts for 5-10% of all PCI procedures performed in current clinical practice. This State-of-the-Art review will primarily focus on the management of ISR but will begin by briefly discussing diagnosis and classification. We then move on to detail the evidence base underpinning the various therapeutic strategies for ISR before finishing with a proposed ISR management algorithm based on current scientific data.
Figures
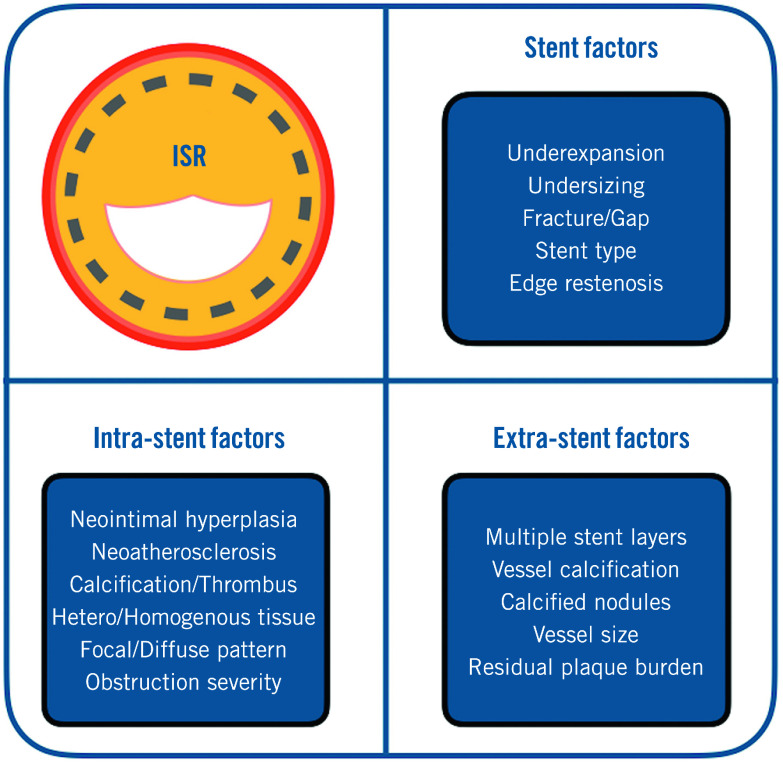
ISR: in-stent restenosis; PCI: percutaneous coronary intervention
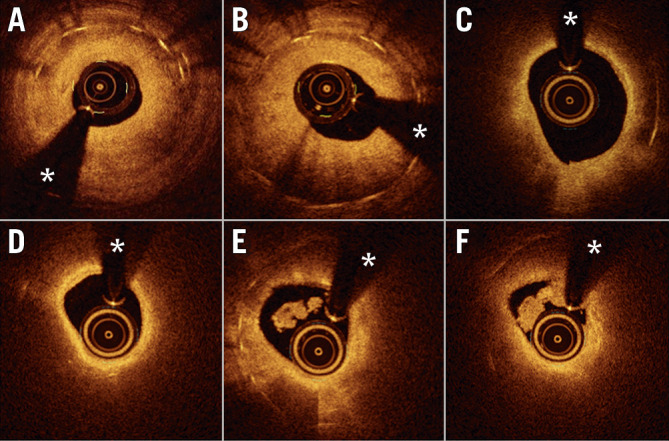
A - B) Demonstrate relatively homogeneous severe neointimal proliferation with some confined darker areas close to the underlying stent struts that are readily visualised (bright dots casting a dorsal shadow). C - F) Typical images of neoatherosclerosis. In C and D, a bright superficial intima and a large lipid plaque (dark area with diffuse borders) is demonstrated obscuring the underlying stent struts. A potential diagnosis of an intimal layer infiltrated by macrophages should be considered. In E and F, neoatherosclerosis with intracoronary thrombus is demonstrated. In E, the bright localised image with dorsal shadow (6-7 o’clock) is suggestive of clusters of macrophages. (* denotes wire artefact). ISR: in-stent restenosis; OCT: optical coherence tomography
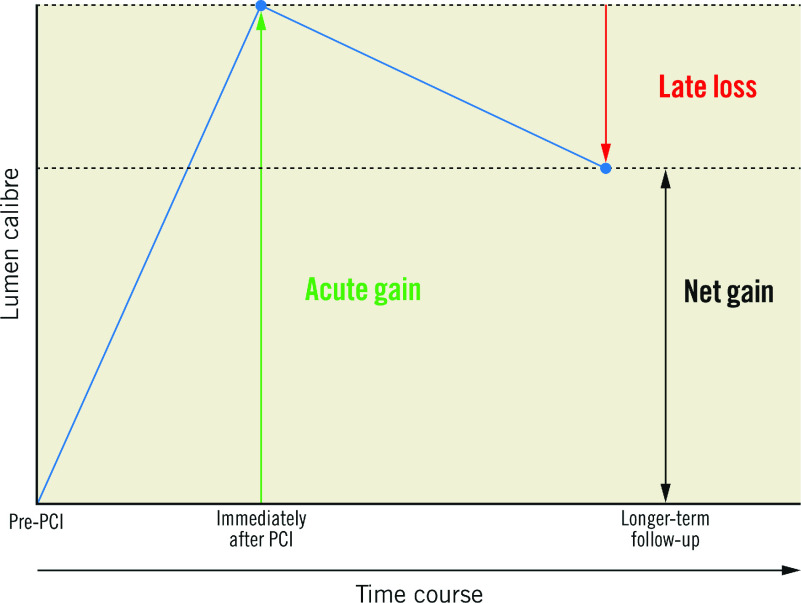
When treating ISR, the aim is to maximise acute gain and minimise LLL. The most important parameter when comparing DESs and DCBs for the treatment of ISR is net gain. DES: drug-eluting stent; DCB: drug-coated balloon; ISR: in-stent restenosis; LLL: late lumen loss; PCI: percutaneous coronary intervention
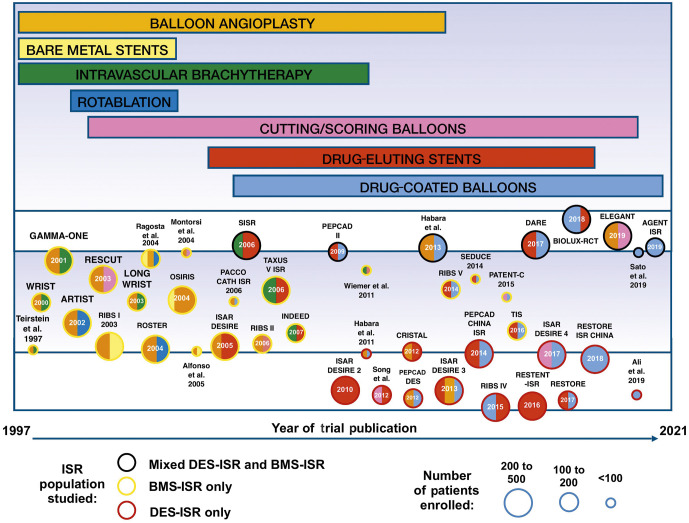
The size of the circles corresponds to the size of the trial. The colour of the circles’ perimeter indicates the underlying stent type in the ISR population studied. The inner colour of the circle indicates the interventional strategies used in the trial, corresponding to the coloured bars at the top of the figure. The length of the coloured bars at the top of the figure indicates the time span during which each therapeutic modality has been studied for the treatment of ISR. Detailed descriptions of the studies and the randomised arms are provided in Supplementary Table 1. BMS: bare metal stent; DES: drug-eluting stent; ISR: in-stent restenosis
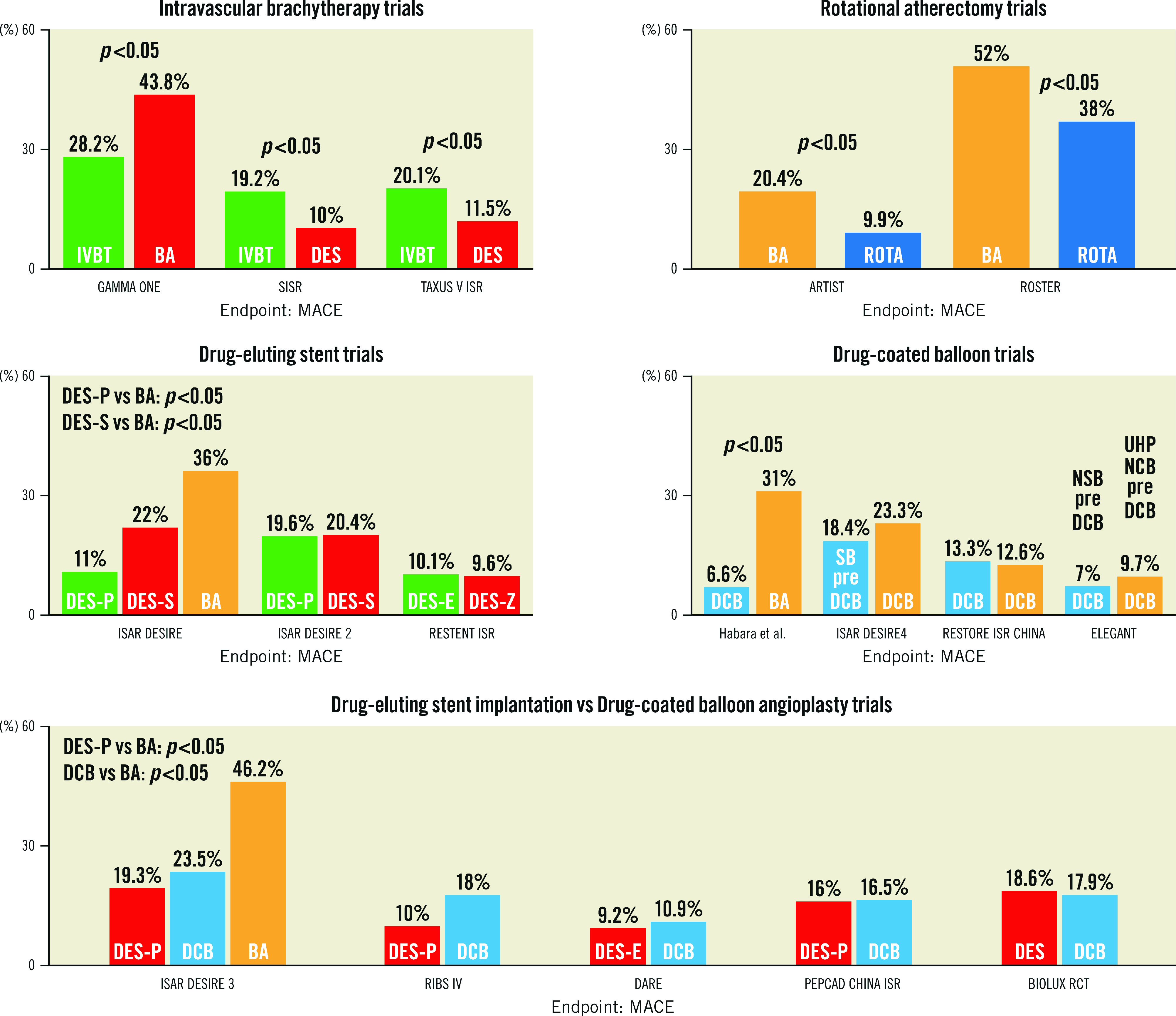
ISR trials with over 200 patients enrolled are divided into 5 research themes: intravascular brachytherapy trials, rotational atherectomy trials, DES trials, DCB trials, and DES vs DCB trials. MACE is the outcome of interest displayed for each trial. Three ISR trials with >200 patients enrolled are not shown in this figure: These are RIBS I (Bare Metal Stent vs Balloon Angioplasty), RESCUT (Balloon Angioplasty vs Cutting Balloon) and OSIRIS (Placebo vs Normal Dose Sirolimus vs High Dose Sirolimus). Details of all ISR trials identified in our search are provided in Supplementary Table 1 and Supplementary Table 2. BA: balloon angioplasty; DCB: drug-coated balloons; DES: drug-eluting stent; DES-E: everolimus-eluting stent; DES-P: paclitaxel-eluting stent; DES-S: sirolimus-eluting stent; DES-Z: zotarolimus-eluting stent; ISR: in-stent restenosis; IVBT: intravascular brachytherapy; MACE: major adverse cardiac events; NSB: non-slip balloon: SB:scoring balloon; UHPNCB: ultra-high-pressure non-compliant balloon
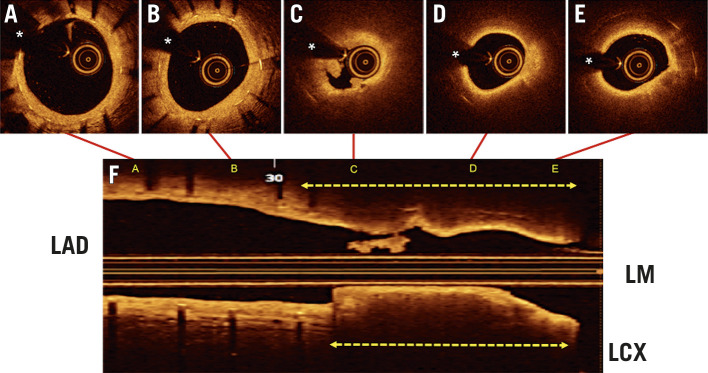
The ECG was normal but a rise in high-sensitivity troponins was detected. A-E) OCT images from the distal part of the stent (A) to the LAD ostium (E) are shown. F) The longitudinal OCT display depicting the location of the corresponding cross-sections. The distal part of the stent (A, B) showed a mild neointimal hyperplasia (with a homogeneous bright yellow colour) and an excellent residual coronary lumen (* denotes wire artefact). Alternatively, the proximal part of the stent (C-D) showed ruptured neoatherosclerosis with intracoronary thrombus (C, F). There is a ruptured cap with associated thrombus (C) and bright neointima (D,E) overlying a large lipid plaque (dark areas with undefined edges), which completely obscure (shadowing) most of the underlying stent struts. The broken arrows indicate the area which demonstrates obstructive neoatherosclerosis (F). DES: drug-eluting stent; ECG: electrocardiogram; ISR: in-stent restenosis; LAD: left anterior descending coronary artery; LCX: left circumflex coronary artery; LM: left main; OCT: optical coherence tomography
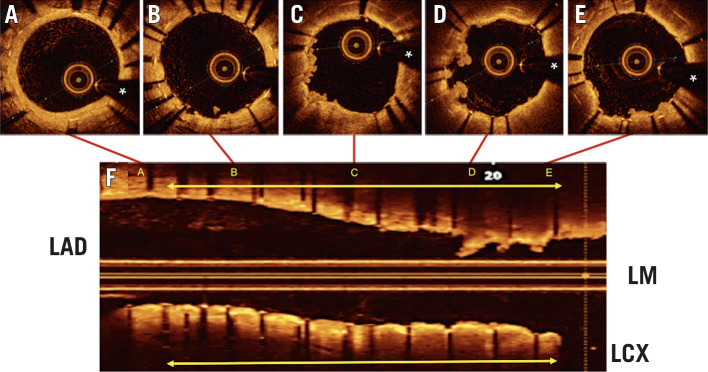
The location of the cross-section images (A-E, top) is illustrated in the longitudinal display (F, bottom). A) Distal untreated segment of the previous stent. B-E) Treated segment (yellow arrow) demonstrating the 2 stent layers. There is also a significant protrusion of soft irregular material into the coronary lumen. (* denotes wire artefact). DES: drug-eluting stent; ISR: in-stent restenosis; LAD: left anterior descending coronary artery; LCX: left circumflex coronary artery; LM: left main; OCT: optical coherence tomography
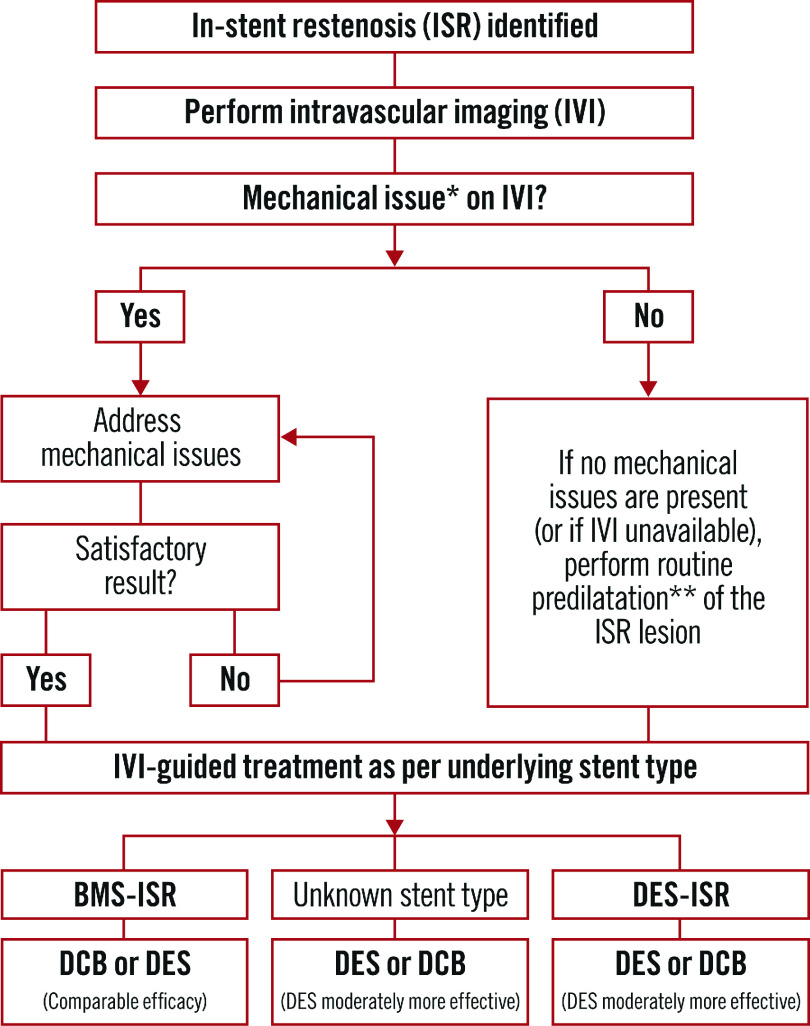
*Mechanical issues can include stent undersizing, stent underexpansion, vessel calcification, stent fracture, and geographic miss. Mechanical issues can be addressed via a variety of methods dependent on the identified pathology and local skill set. These methods can include BA, RA, ELCA, IVL, UHPNCB, cutting, and scoring balloons. **Predilatation can be performed with BA, UHPNCB, cutting, or scoring balloons. Cutting and scoring balloons may be particularly useful prior to planned DCB therapy. BA: balloon angioplasty; BMS: bare metal stent; DCB: drug-coated balloon; DES: drug-eluting stent; ELCA: excimer laser coronary atherectomy; ISR: in-stent restenosis; IVI: intravascular imaging; IVL: intravascular lithotripsy; RA: rotational atherectomy; UHPNCB: ultra-high-pressure non-compliant balloons
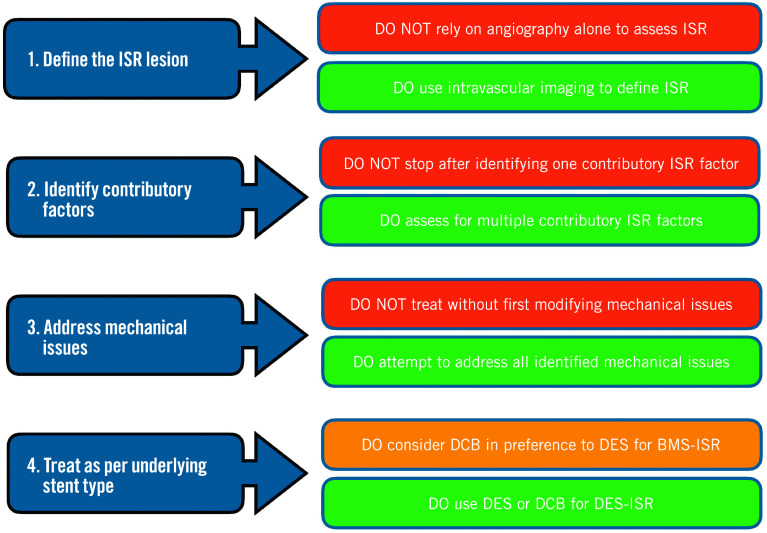
BMS: bare metal stent; DCB: drug-coated balloon; DES: drug-eluting stent; ISR: in-stent restenosis; PCI: percutaneous coronary intervention
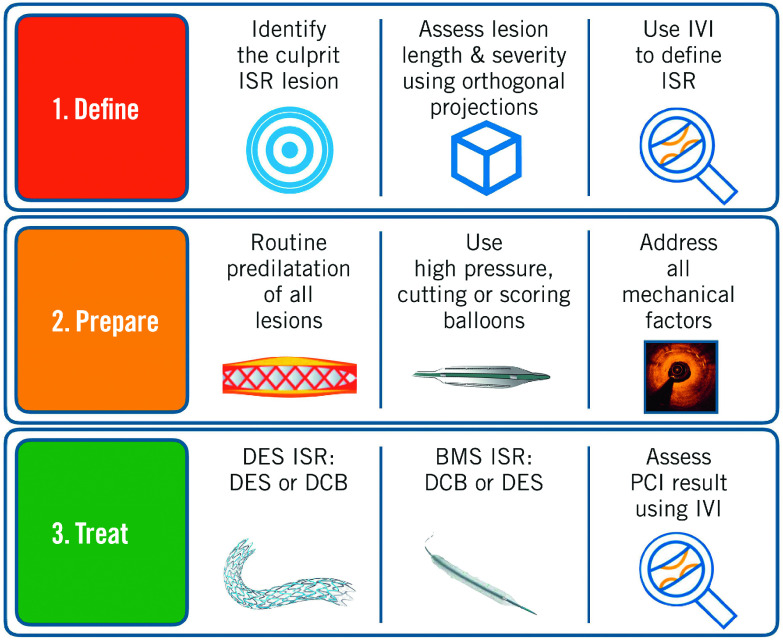
First, the ISR lesion should be identified and defined using IVI. The lesion should then be prepared using balloon dilatation. High-pressure, cutting or scoring balloons can be used as required. Mechanical factors contributing to ISR should be addressed. This may require adjunctive modalities, including RA, ELCA, and IVL, depending on local expertise. Once the lesion has been adequately prepared, treatment with a DES or DCB should be used for the majority of cases. DESs are moderately more effective than DCBs in DES-ISR. For BMS-ISR, DCBs and DESs are comparatively effective and so DCBs should be considered preferentially. After PCI, IVI should be considered to confirm a satisfactory result has been achieved. BMS: bare metal stent; DCB: drug-coated balloon; DES: drug-eluting stent; ELCA: excimer laser coronary atherectomy; ISR: in-stent restenosis; IVI: intravascular imaging; IVL: intravascular lithotripsy; PCI: percutaneous coronary intervention; RA: rotational atherectomy
References
-
- Dangas GD, Claessen BE, Caixeta A, Sanidas EA, Mintz GS, Mehran R. In-stent restenosis in the drug-eluting stent era. J Am Coll Cardiol. 2010;56:1897–907. - PubMed
-
- Alfonso F, Byrne RA, Rivero F, Kastrati A. Current treatment of in-stent restenosis. J Am Coll Cardiol. 2014;63:2659–73. - PubMed
-
- Kastrati A, Mehilli J, Pache J, Kaiser C, Valgimigli M, Kelbaek H, Menichelli M, Sabaté M, Suttorp MJ, Baumgart D, Seyfarth M, Pfisterer ME, Schömig A. Analysis of 14 trials comparing sirolimus-eluting stents with bare-metal stents. N Engl J Med. 2007;356:1030–9. - PubMed
-
- Stettler C, Wandel S, Allemann S, Kastrati A, Morice MC, Schömig A, Pfisterer ME, Stone GW, Leon MB, de Lezo, Goy JJ, Park SJ, Sabaté M, Suttorp MJ, Kelbaek H, Spaulding C, Menichelli M, Vermeersch P, Dirksen MT, Cervinka P, Petronio AS, Nordmann AJ, Diem P, Meier B, Zwahlen M, Reichenbach S, Trelle S, Windecker S, Jüni P. Outcomes associated with drug-eluting and bare-metal stents: a collaborative network meta-analysis. Lancet. 2007;370:937–48. - PubMed
-
- Moussa ID, Mohananey D, Saucedo J, Stone GW, Yeh RW, Kennedy KF, Waksman R, Teirstein P, Moses JW, Simonton C. Trends and Outcomes of Restenosis After Coronary Stent Implantation in the United States. J Am Coll Cardiol. 2020;76:1521–31. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous