

Amiodarone Use and All-Cause Mortality in Patients With a Continuous-Flow Left Ventricular Assist Device
- PMID: 35656998
- PMCID: PMC9238747
- DOI: 10.1161/JAHA.121.023762
Amiodarone Use and All-Cause Mortality in Patients With a Continuous-Flow Left Ventricular Assist Device
Abstract
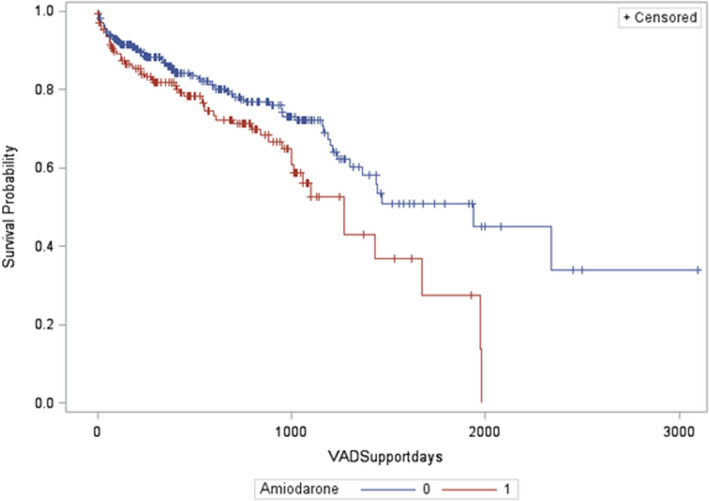
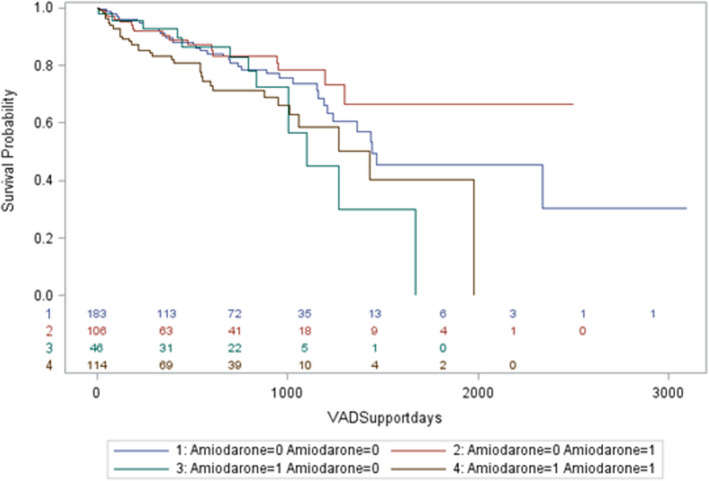
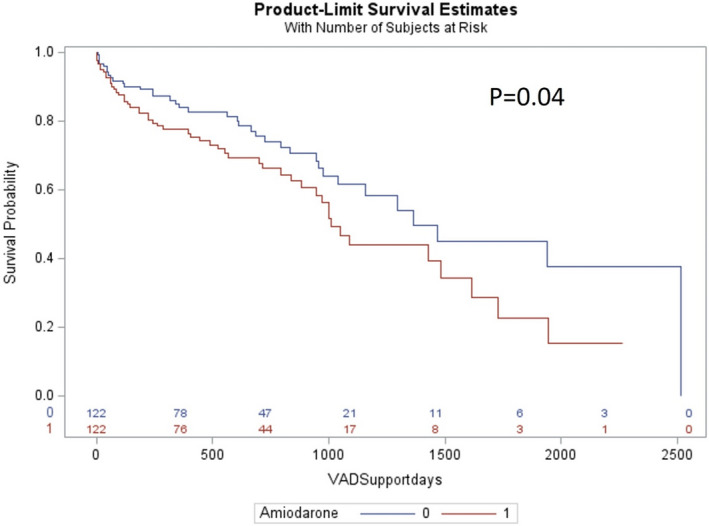
Background Atrial and ventricular arrhythmias are commonly encountered in patients with advanced heart failure, with amiodarone being the most commonly used antiarrhythmic drug in continuous-flow left ventricular assist device (CF-LVAD) recipients. The purpose of this study was to assess the impact of amiodarone use on long-term all-cause mortality in ptients with a CF-LVAD. Methods and Results A retrospective multicenter study of CF-LVAD was conducted at 5 centers including all CF-LVAD implants from 2007 to 2015. Patients were stratified based on pre-CF-LVAD implant amiodarone use. Additional use of amiodarone after CF-LVAD implantation was also evaluated. Primary outcome was all-cause mortality during long-term follow-up. Kaplan-Meier curves were used to assess survival outcomes. Multivariable Cox regression was used to identify predictors of outcomes. Propensity matching was done to address baseline differences. A total of 480 patients with a CF-LVAD (aged 58±13 years, 81% men) were included. Of these, 170 (35.4%) were on chronic amiodarone therapy at the time of CF-LVAD implant, and 310 (64.6%) were not on amiodarone. Rate of all-cause mortality over the follow-up period was 32.9% in the amiodarone group compared with 29.6% in those not on amiodarone (P=0.008). Similar results were noted in the propensity-matched group (log-rank, P=0.04). On multivariable Cox regression analysis, amiodarone use at baseline was independently associated with all-cause mortality (hazard ratio, 1.68 [95% CI, 1.1-2.5]; P=0.01). Conclusions Amiodarone use was associated with significantly increased rates of all-cause mortality in CF-LVAD recipients. Earlier interventions for arrhythmias to avoid long-term amiodarone exposure may improve long-term outcomes in CF-LVAD recipients and needs further study.
Keywords: amiodarone; arrhythmias; left ventricular assist device; mortality.
Figures
References
-
- Hohnloser SH, Dorian P, Roberts R, Gent M, Israel CW, Fain E, Champagne J, Connolly SJ. Effect of amiodarone and sotalol on ventricular defibrillation threshold: the optimal pharmacological therapy in cardioverter defibrillator patients (OPTIC) trial. Circulation. 2006;114:104–109. doi: 10.1161/CIRCULATIONAHA.106.618421 - DOI - PubMed
-
- Connolly SJ, Hallstrom AP, Cappato R, Schron EB, Kuck KH, Zipes DP, Greene HL, Boczor S, Domanski M, Follmann D, et al. Meta‐analysis of the implantable cardioverter defibrillator secondary prevention trials. AVID, CASH and CIDS studies. Antiarrhythmics vs Implantable Defibrillator study. Cardiac Arrest Study Hamburg. Canadian Implantable Defibrillator Study. Eur Heart J. 2000;21:2071–2078. doi: 10.1053/euhj.2000.2476 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
