

Two-day versus seven-day course of levofloxacin in acute COPD exacerbation: a randomized controlled trial
- PMID: 35657073
- PMCID: PMC9168850
- DOI: 10.1177/17534666221099729
Two-day versus seven-day course of levofloxacin in acute COPD exacerbation: a randomized controlled trial
Retraction in
-
Retraction: "Two-day versus seven-day course of levofloxacin in acute COPD exacerbation: a randomized controlled trial".Ther Adv Respir Dis. 2025 Jan-Dec;19:17534666251362671. doi: 10.1177/17534666251362671. Epub 2025 Jul 30. Ther Adv Respir Dis. 2025. PMID: 40739462 Free PMC article. No abstract available.
Expression of concern in
-
Expression of concern: 'Two-day versus seven-day course of levofloxacin in acute COPD exacerbation: a randomized controlled trial'.Ther Adv Respir Dis. 2023 Jan-Dec;17:17534666231190750. doi: 10.1177/17534666231190750. Ther Adv Respir Dis. 2023. PMID: 37571965 Free PMC article. No abstract available.
Abstract
Introduction: Duration of antibiotic treatment in acute exacerbation of COPD (AECOPD) is most commonly based on expert opinion. Typical administration periods range from 5 to 7 days. A 2-day course with levofloxacin was not previously assessed. We performed a randomized clinical trial to evaluate the efficacy of 2-day versus 7-day treatment with levofloxacin in patients with AECOPD.
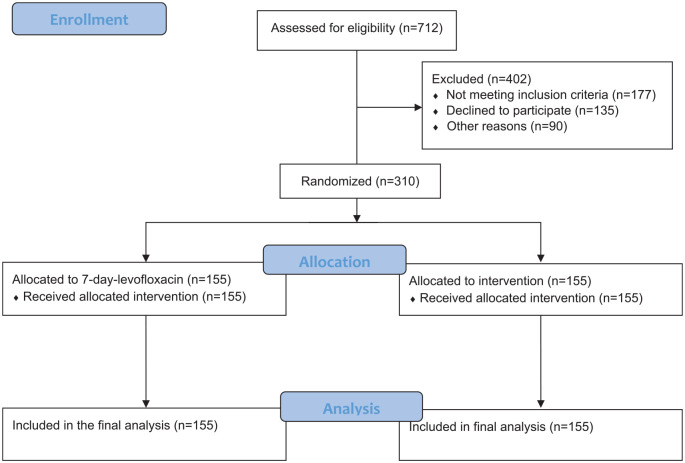
Methods and analysis: Patients with AECOPD were randomized to receive levofloxacin for 2 days and 5 days placebo (n = 155) or levofloxacin for 7 days (n = 155). All patients received a common dose of intravenous prednisone daily for 5 days. The primary outcome measure was cure rate, and secondary outcomes included need for additional antibiotics, ICU admission rate, re-exacerbation rate, death rate, and exacerbation-free interval (EFI) within 1-year follow-up. The study protocol has been prepared in accordance with the revised Helsinki Declaration for Biomedical Research Involving Human Subjects and Guidelines for Good Clinical Practice. The study was approved by ethics committees of all participating centers prior to implementation (Monastir and Sousse Universities).
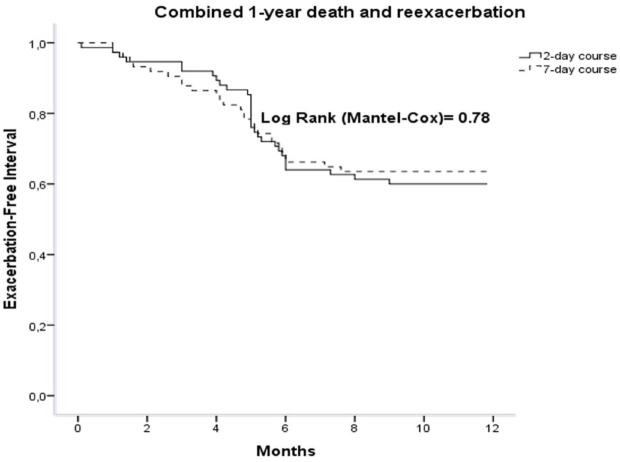
Results: 310 patients were randomized to receive 2-day course of levofloxacin (n = 155) or 7-day course (n = 155). Cure rate was 79.3% (n = 123) and 74.2% (n = 115), respectively, in 2-day and 7-day groups [OR 1.3; 95% CI 0.78-2.2 (p = 0.28)]. Need for additional antibiotics rate was 3.2% and 1.9% in the 2-day group and 7-day group, respectively; (p = 0.43). ICU admission rate was not significantly different between both groups. One-year re-exacerbation rate was 34.8% (n = 54) in 2-day group versus 29% (n = 45) in 7-day group (p = 0.19); the EFI was 121 days (interquartile range, 99-149) versus 110 days (interquartile range, 89-132) in 2-day and 7-day treatment groups, respectively; (p = 0.73). One-year death rate was not significantly different between the 2 groups, 5.2% versus 7.1% in the 2-day group and 7-day group, respectively; (p = 0.26). No difference in adverse effects was detected.
Conclusion: Levofloxacin once daily for 2 days is not inferior to 7 days with respect to cure rate, need for additional antibiotics and hospital readmission in AECOPD. Our findings would improve patient compliance and reduce the incidence of bacterial resistance and adverse effects.
Keywords: acute exacerbation of COPD; levofloxacin; short course antibiotics.
Conflict of interest statement
Figures
References
-
- Vogelmeier CF, Criner GJ, Martinez FJ. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med 2017; 195: 557–582. - PubMed
-
- Jacobs DM, Pandit U, Sethi S. Acute exacerbations in chronic obstructive pulmonary disease: should we use antibiotics and if so, which ones. Curr Opin Infect Dis 2019; 32: 143–151. - PubMed
-
- Desai H, Richter S, Doern G, et al. Antibiotic resistance in sputum isolates of Streptococcus pneumoniae in chronic obstructive pulmonary disease is related to antibiotic exposure. COPD 2010; 7: 33744. - PubMed
-
- Papi A, Bellettato CM, Braccioni F, et al. Infections and airway inflammation in chronic obstructive pulmonary disease severe exacerbations. Am J Respir Crit Care Med 2006; 173: 111421. - PubMed
-
- Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med 2011; 184: 66271. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
