

Association of Bariatric Surgery With Cancer Risk and Mortality in Adults With Obesity
- PMID: 35657620
- PMCID: PMC9166218
- DOI: 10.1001/jama.2022.9009
Association of Bariatric Surgery With Cancer Risk and Mortality in Adults With Obesity
Abstract
Importance: Obesity increases the incidence and mortality from some types of cancer, but it remains uncertain whether intentional weight loss can decrease this risk.
Objective: To investigate whether bariatric surgery is associated with lower cancer risk and mortality in patients with obesity.
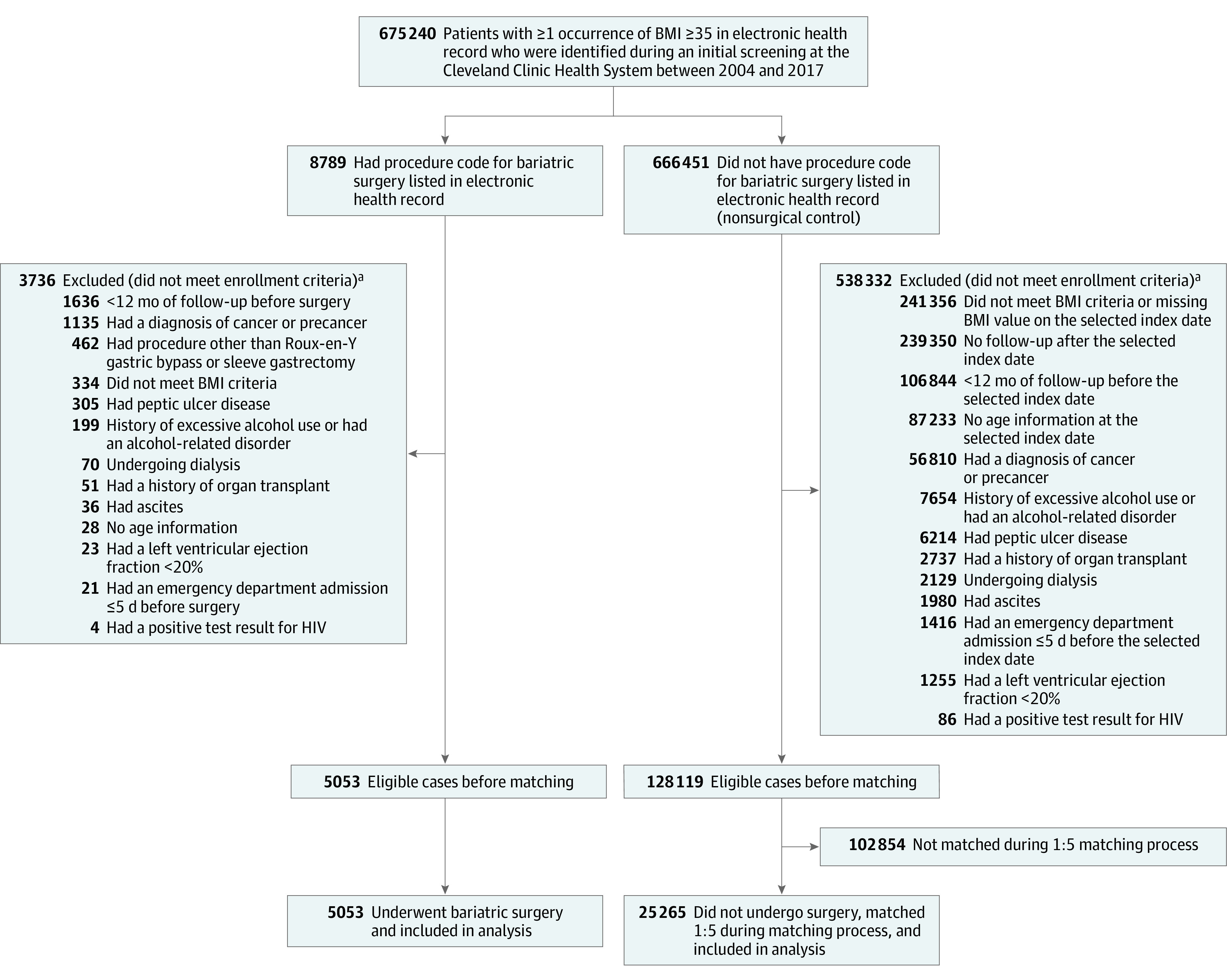
Design, setting, and participants: In the SPLENDID (Surgical Procedures and Long-term Effectiveness in Neoplastic Disease Incidence and Death) matched cohort study, adult patients with a body mass index of 35 or greater who underwent bariatric surgery at a US health system between 2004 and 2017 were included. Patients who underwent bariatric surgery were matched 1:5 to patients who did not undergo surgery for their obesity, resulting in a total of 30 318 patients. Follow-up ended in February 2021.
Exposures: Bariatric surgery (n = 5053), including Roux-en-Y gastric bypass and sleeve gastrectomy, vs nonsurgical care (n = 25 265).
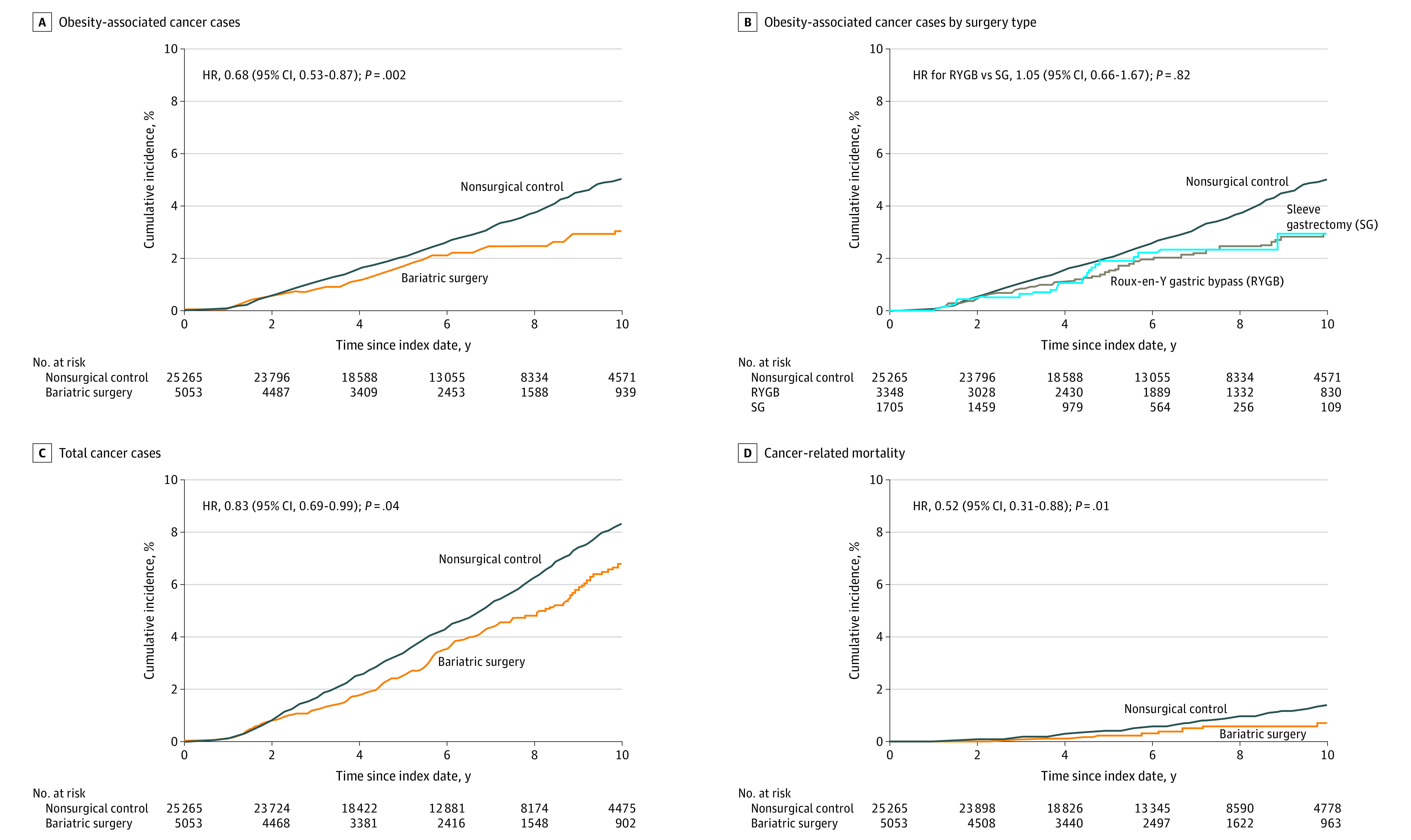
Main outcomes and measures: Multivariable Cox regression analysis estimated time to incident obesity-associated cancer (a composite of 13 cancer types as the primary end point) and cancer-related mortality.
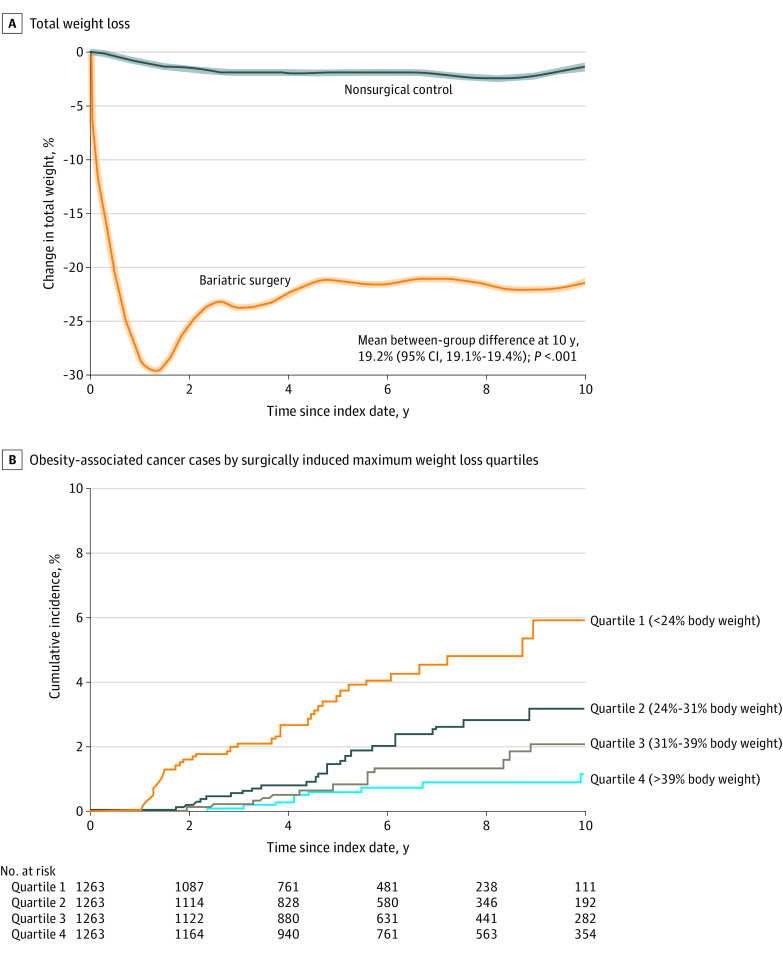
Results: The study included 30 318 patients (median age, 46 years; median body mass index, 45; 77% female; and 73% White) with a median follow-up of 6.1 years (IQR, 3.8-8.9 years). The mean between-group difference in body weight at 10 years was 24.8 kg (95% CI, 24.6-25.1 kg) or a 19.2% (95% CI, 19.1%-19.4%) greater weight loss in the bariatric surgery group. During follow-up, 96 patients in the bariatric surgery group and 780 patients in the nonsurgical control group had an incident obesity-associated cancer (incidence rate of 3.0 events vs 4.6 events, respectively, per 1000 person-years). The cumulative incidence of the primary end point at 10 years was 2.9% (95% CI, 2.2%-3.6%) in the bariatric surgery group and 4.9% (95% CI, 4.5%-5.3%) in the nonsurgical control group (absolute risk difference, 2.0% [95% CI, 1.2%-2.7%]; adjusted hazard ratio, 0.68 [95% CI, 0.53-0.87], P = .002). Cancer-related mortality occurred in 21 patients in the bariatric surgery group and 205 patients in the nonsurgical control group (incidence rate of 0.6 events vs 1.2 events, respectively, per 1000 person-years). The cumulative incidence of cancer-related mortality at 10 years was 0.8% (95% CI, 0.4%-1.2%) in the bariatric surgery group and 1.4% (95% CI, 1.1%-1.6%) in the nonsurgical control group (absolute risk difference, 0.6% [95% CI, 0.1%-1.0%]; adjusted hazard ratio, 0.52 [95% CI, 0.31-0.88], P = .01).
Conclusions and relevance: Among adults with obesity, bariatric surgery compared with no surgery was associated with a significantly lower incidence of obesity-associated cancer and cancer-related mortality.
Conflict of interest statement
Figures
Comment in
-
Bariatric Surgery and Cancer Risk.JAMA. 2022 Jun 28;327(24):2400-2402. doi: 10.1001/jama.2022.9166. JAMA. 2022. PMID: 35657635 No abstract available.
-
Cancer Risk Following Bariatric Surgery.Gastroenterology. 2022 Dec;163(6):1713-1714. doi: 10.1053/j.gastro.2022.08.029. Epub 2022 Aug 17. Gastroenterology. 2022. PMID: 35987444 No abstract available.
-
Association of Bariatric Surgery With Cancer Risk and Mortality.JAMA. 2022 Oct 25;328(16):1645-1646. doi: 10.1001/jama.2022.16518. JAMA. 2022. PMID: 36282263 No abstract available.
References
-
- Byers T, Sedjo RL. Does intentional weight loss reduce cancer risk? Diabetes Obes Metab. 2011;13(12):1063-1072. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
