

Association of Accelerometer-Measured Sedentary Time and Physical Activity With Risk of Stroke Among US Adults
- PMID: 35657625
- PMCID: PMC9166254
- DOI: 10.1001/jamanetworkopen.2022.15385
Association of Accelerometer-Measured Sedentary Time and Physical Activity With Risk of Stroke Among US Adults
Abstract
Importance: The amount and intensity of physical activity required to prevent stroke are yet to be fully determined because of previous reliance on self-reporting measures. Furthermore, the association between objectively measured time spent being sedentary as an independent risk factor for stroke is unknown.
Objective: To investigate the associations of accelerometer-measured sedentary time and physical activity of varying intensity and duration with the risk of incident stroke.
Design, setting, and participants: This cohort study involved participants who were enrolled in the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study from February 5, 2003, to October 30, 2007. Accelerometer data were collected from 7607 Black and White adults 45 years or older in the contiguous US between May 12, 2009, and January 5, 2013. Data on other races and ethnicities were not collected for scientific and clinical reasons. By design, Black adults and residents of the southeastern US stroke belt and stroke buckle were oversampled. Data were analyzed from May 5, 2020, to November 11, 2021.
Exposures: Sedentary time, light-intensity physical activity (LIPA), and moderate- to vigorous-intensity physical activity (MVPA) were measured using a hip-mounted accelerometer worn for 7 consecutive days and stratified by tertile for the analyses.
Main outcomes and measures: Incident stroke.
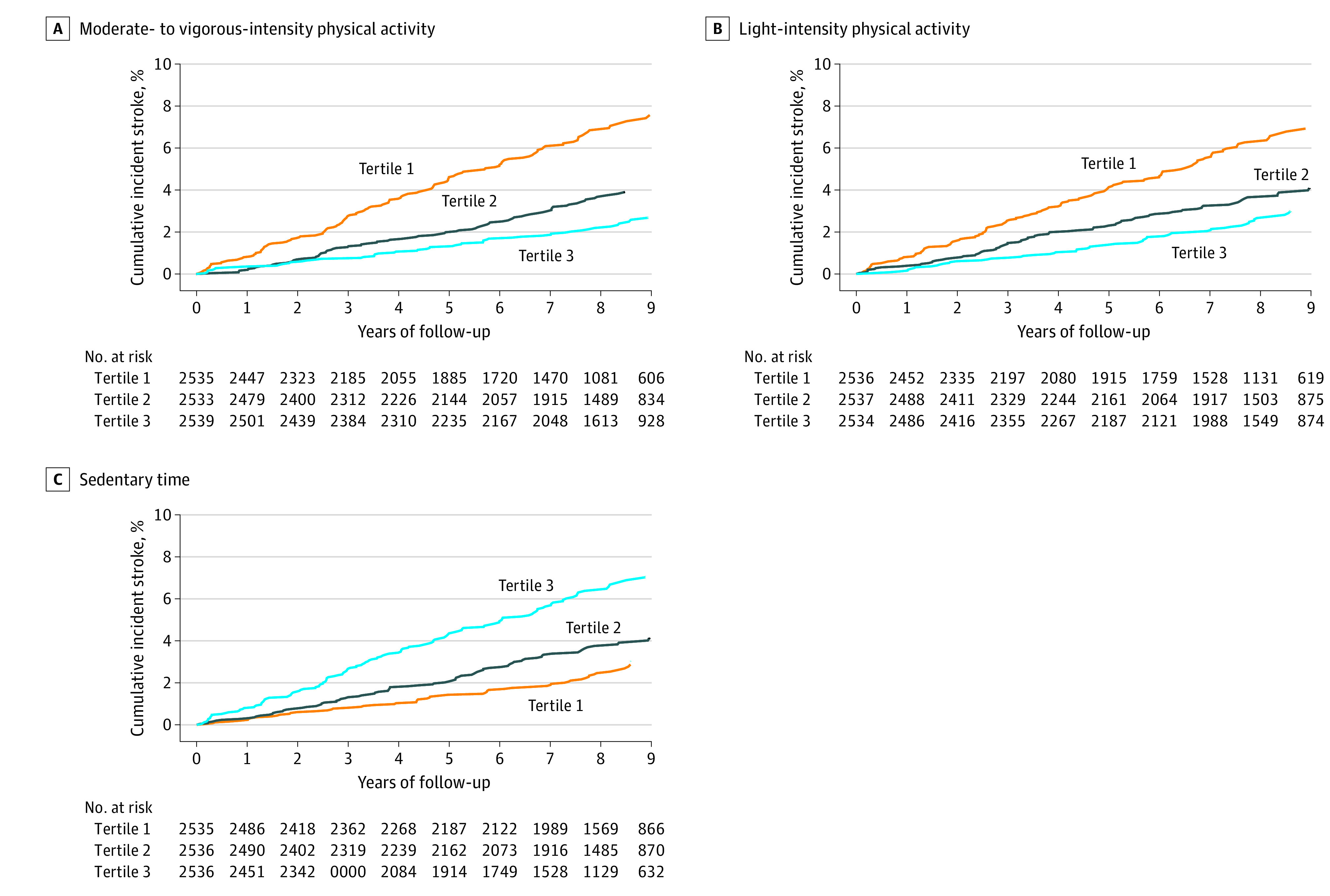
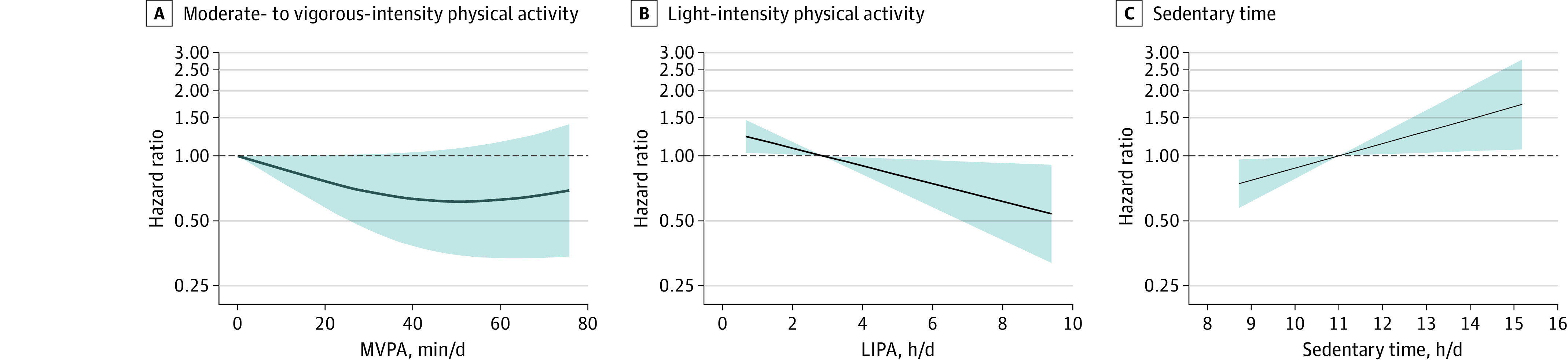
Results: Among 7607 participants, the mean (SD) age was 63.4 (8.5) years; 4145 participants (54.5%) were female, 2407 (31.6%) were Black, and 5200 (68.4%) were White. A total of 2523 participants (33.2%) resided in the stroke belt, and 1638 (21.5%) resided in the stroke buckle. Over a mean (SD) of 7.4 (2.5) years of follow-up, 286 incident stroke cases (244 ischemic [85.3%]) occurred. The fully adjusted hazard ratios (HRs) for incident stroke in the highest tertile compared with the lowest tertile were 0.74 (95% CI, 0.53-1.04; P = .08) for LIPA and 0.57 (95% CI, 0.38-0.84; P = .004) for MVPA. Higher sedentary time was associated with a 44% greater risk of incident stroke (HR, 1.44; 95% CI, 0.99-2.07; P = .04). When comparing the highest with the lowest tertile, mean sedentary bout duration was associated with a significantly greater risk of incident stroke (HR, 1.53; 95% CI, 1.10-2.12; P = .008). After adjustment for sedentary time, the highest tertile of unbouted MVPA (shorter bouts [1-9 minutes]) was associated with a significantly lower risk of incident stroke compared with the lowest tertile (HR, 0.62; 95% CI, 0.41-0.94; P = .02); however, bouted MVPA (longer bouts [at least 10 minutes]) was not (HR, 0.78; 95% CI, 0.53-1.15; P = .17). When expressed as continuous variables, sedentary time was positively associated with incident stroke risk (HR per 1-hour/day increase in sedentary time: 1.14; 95% CI, 1.02-1.28; P = .02), and LIPA was negatively associated with incident stroke risk (HR per 1-hour/day increase in LIPA: 0.86; 95% CI, 0.77-0.97; P = .02).
Conclusions and relevance: In this cohort study, objectively measured LIPA, MVPA, and sedentary time were significantly and independently associated with incident stroke risk. Longer sedentary bout duration was also independently associated with an increased risk of incident stroke. These findings suggest that replacing sedentary time with LIPA, or even very short bouts of MVPA, may lower stroke risk, supporting the concept of moving more and sitting less as a beneficial stroke risk reduction strategy among adults.
Conflict of interest statement
Figures
References
-
- Virani SS, Alonso A, Aparicio HJ, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2021 update: a report from the American Heart Association. Circulation. 2021;143(8):e254-e743. doi:10.1161/CIR.0000000000000950 - DOI - PubMed
-
- Meschia JF, Bushnell C, Boden-Albala B, et al. ; American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Functional Genomics and Translational Biology; Council on Hypertension . Guidelines for the primary prevention of stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(12):3754-3832. doi:10.1161/STR.0000000000000046 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
