

Longitudinal kinetics of RBD+ antibodies in COVID-19 recovered patients over 14 months
- PMID: 35658051
- PMCID: PMC9200310
- DOI: 10.1371/journal.ppat.1010569
Longitudinal kinetics of RBD+ antibodies in COVID-19 recovered patients over 14 months
Abstract
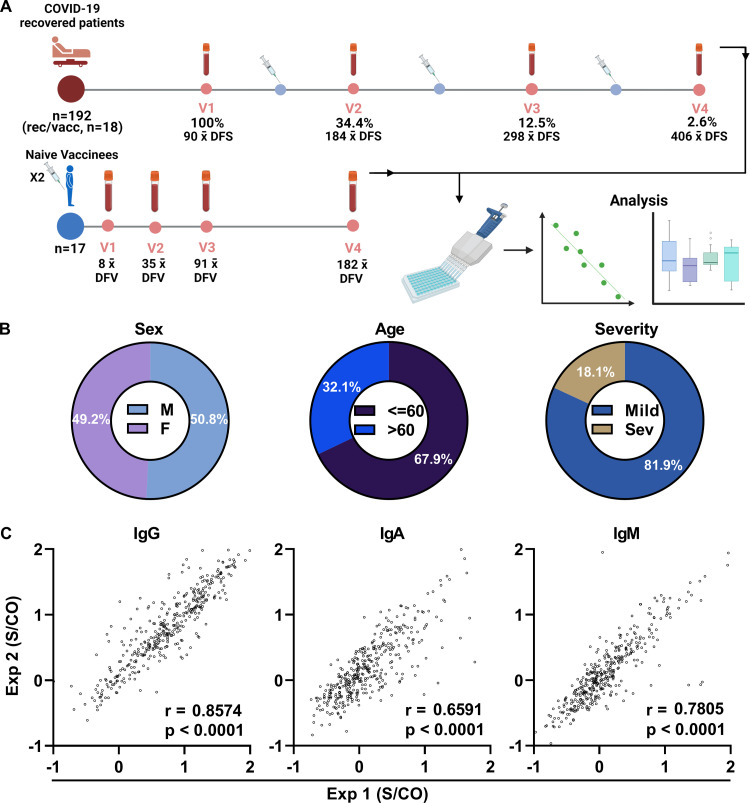
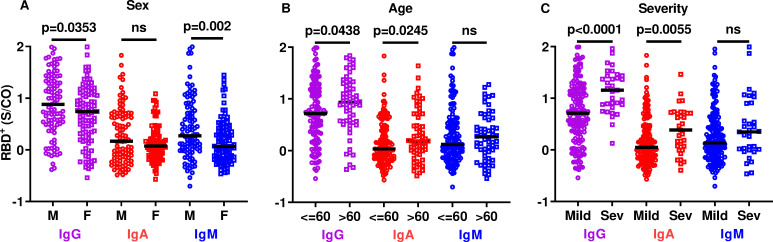
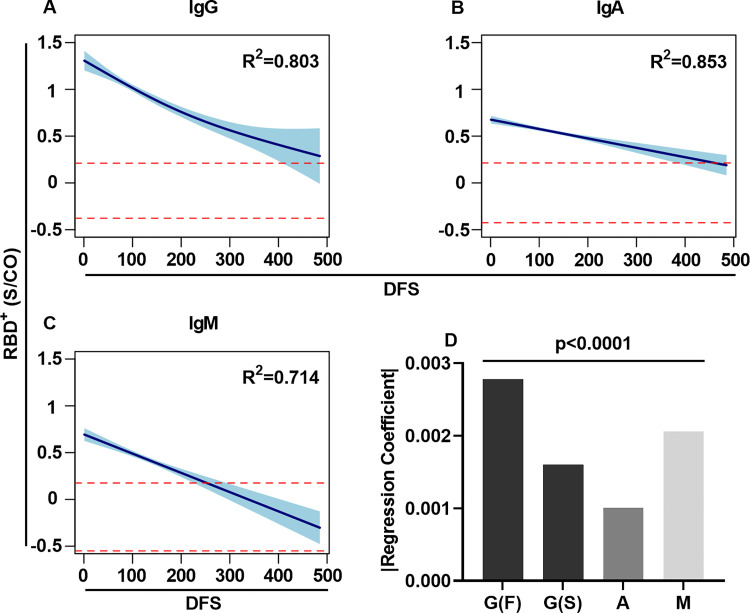
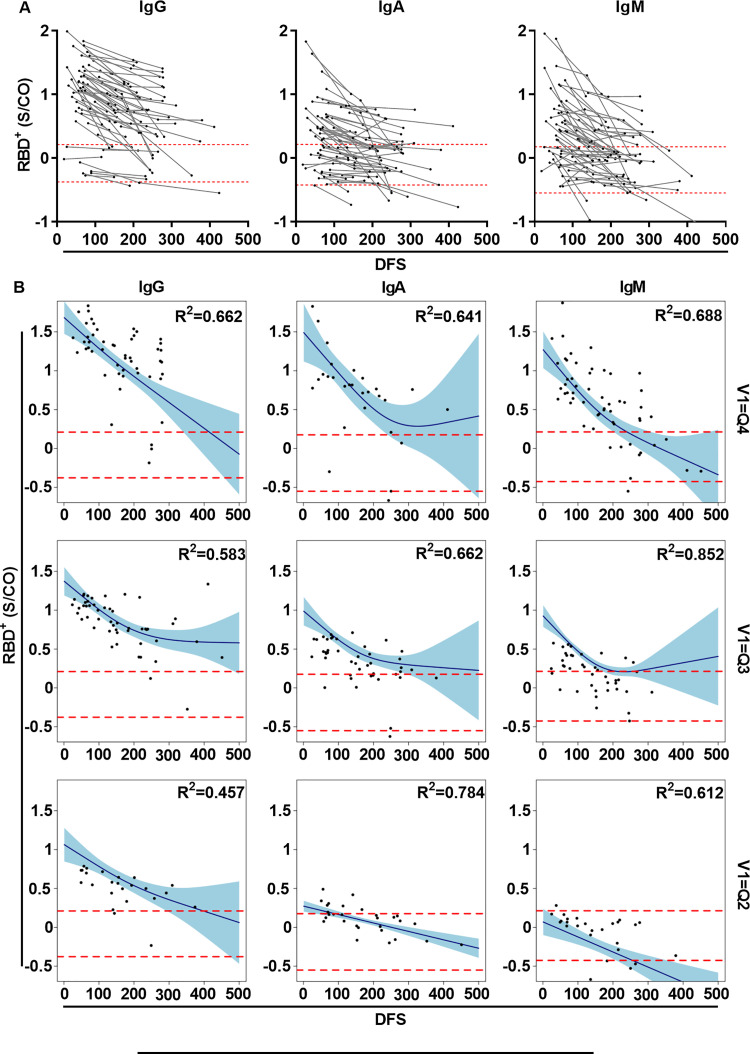
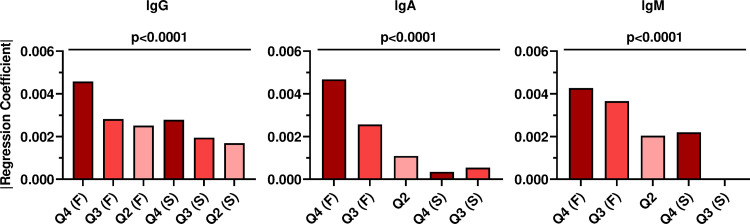
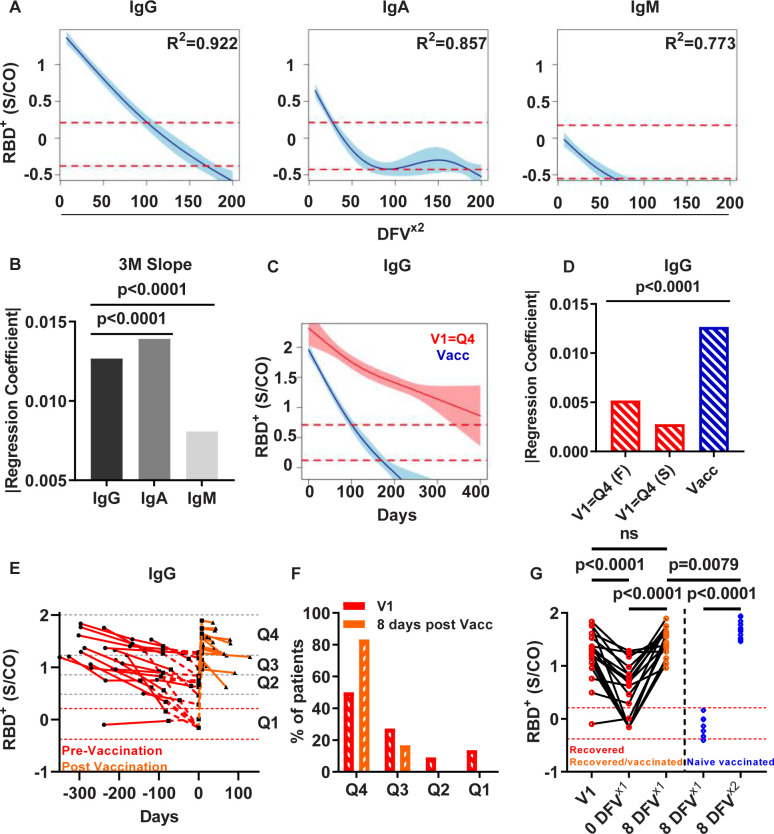
We describe the longitudinal kinetics of the serological response in COVID-19 recovered patients over a period of 14 months. The antibody kinetics in a cohort of 192 recovered patients, including 66 patients for whom follow-up serum samples were obtained at two to four clinic visits, revealed that RBD-specific antibodies decayed over the 14 months following the onset of symptoms. The decay rate was associated with the robustness of the response in that antibody levels that were initially highly elevated after the onset of symptoms subsequently decayed more rapidly. An exploration of the differences in the longitudinal kinetics between recovered patients and naïve vaccinees who had received two doses of the BNT162b2 vaccine showed a significantly faster decay in the naïve vaccinees, indicating that serological memory following natural infection is more robust than that following to vaccination. Our data highlighting the differences between serological memory induced by natural infection vs. vaccination contributed to the decision-making process in Israel regarding the necessity for a third vaccination dose.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Comparative kinetics of SARS-CoV-2 anti-spike protein RBD IgGs and neutralizing antibodies in convalescent and naïve recipients of the BNT162b2 mRNA vaccine versus COVID-19 patients.BMC Med. 2021 Aug 23;19(1):208. doi: 10.1186/s12916-021-02090-6. BMC Med. 2021. PMID: 34420521 Free PMC article.
-
BNT162b2 COVID-19 vaccine and correlates of humoral immune responses and dynamics: a prospective, single-centre, longitudinal cohort study in health-care workers.Lancet Respir Med. 2021 Sep;9(9):999-1009. doi: 10.1016/S2213-2600(21)00220-4. Epub 2021 Jul 2. Lancet Respir Med. 2021. PMID: 34224675 Free PMC article.
-
Different decay of antibody response and VOC sensitivity in naïve and previously infected subjects at 15 weeks following vaccination with BNT162b2.J Transl Med. 2022 Jan 8;20(1):22. doi: 10.1186/s12967-021-03208-3. J Transl Med. 2022. PMID: 34998405 Free PMC article.
-
Neutralizing antibody titers six months after Comirnaty vaccination: kinetics and comparison with SARS-CoV-2 immunoassays.Clin Chem Lab Med. 2021 Dec 16;60(3):456-463. doi: 10.1515/cclm-2021-1247. Print 2022 Feb 23. Clin Chem Lab Med. 2021. PMID: 34911170
-
Healthcare Workers in South Korea Maintain a SARS-CoV-2 Antibody Response Six Months After Receiving a Second Dose of the BNT162b2 mRNA Vaccine.Front Immunol. 2022 Jan 31;13:827306. doi: 10.3389/fimmu.2022.827306. eCollection 2022. Front Immunol. 2022. PMID: 35173736 Free PMC article.
Cited by
-
Longevity of antibody responses is associated with distinct antigen-specific B cell subsets early after infection.Front Immunol. 2024 Dec 17;15:1505719. doi: 10.3389/fimmu.2024.1505719. eCollection 2024. Front Immunol. 2024. PMID: 39742271 Free PMC article.
-
Effect of host factors and COVID-19 infection on the humoral immune repertoire in treated HIV.JCI Insight. 2023 Mar 8;8(5):e166848. doi: 10.1172/jci.insight.166848. JCI Insight. 2023. PMID: 36805331 Free PMC article.
-
Long term anti-SARS-CoV-2 antibody kinetics and correlate of protection against Omicron BA.1/BA.2 infection.Nat Commun. 2023 May 26;14(1):3032. doi: 10.1038/s41467-023-38744-7. Nat Commun. 2023. PMID: 37230973 Free PMC article.
-
Sustained seropositivity up to 20.5 months after COVID-19.BMC Med. 2022 Oct 13;20(1):379. doi: 10.1186/s12916-022-02570-3. BMC Med. 2022. PMID: 36224590 Free PMC article.
-
Impact of immune evasion, waning and boosting on dynamics of population mixing between a vaccinated majority and unvaccinated minority.PLoS One. 2024 Apr 4;19(4):e0297093. doi: 10.1371/journal.pone.0297093. eCollection 2024. PLoS One. 2024. PMID: 38574059 Free PMC article.
References
-
- Huang AT, Garcia-Carreras B, Hitchings MDT, Yang B, Katzelnick LC, Rattigan SM, et al.. A systematic review of antibody mediated immunity to coronaviruses: kinetics, correlates of protection, and association with severity. Nat Commun. 2020;11(1):4704. doi: 10.1038/s41467-020-18450-4 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
