

Strategies designed to help healthcare professionals to recruit participants to research studies
- PMID: 35658160
- PMCID: PMC8190980
- DOI: 10.1002/14651858.MR000036.pub2
Strategies designed to help healthcare professionals to recruit participants to research studies
Abstract
Background: Identifying and approaching eligible participants for recruitment to research studies usually relies on healthcare professionals. This process is sometimes hampered by deliberate or inadvertent gatekeeping that can introduce bias into patient selection.
Objectives: Our primary objective was to identify and assess the effect of strategies designed to help healthcare professionals to recruit participants to research studies.
Search methods: We performed searches on 5 January 2015 in the following electronic databases: Cochrane Methodology Register, CENTRAL, MEDLINE, EMBASE, CINAHL, British Nursing Index, PsycINFO, ASSIA and Web of Science (SSCI, SCI-EXPANDED) from 1985 onwards. We checked the reference lists of all included studies and relevant review articles and did citation tracking through Web of Science for all included studies.
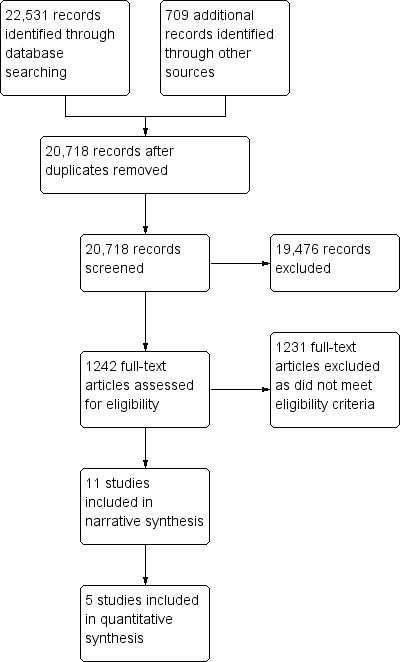
Selection criteria: We selected all studies that evaluated a strategy to identify and recruit participants for research via healthcare professionals and provided pre-post comparison data on recruitment rates.
Data collection and analysis: Two review authors independently screened search results for potential eligibility, read full papers, applied the selection criteria and extracted data. We calculated risk ratios for each study to indicate the effect of each strategy.
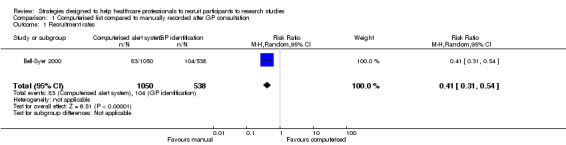
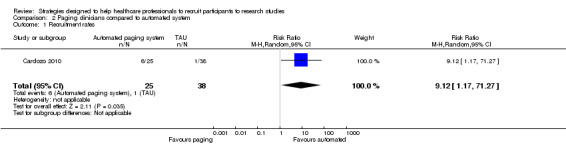
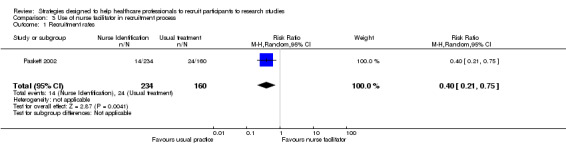
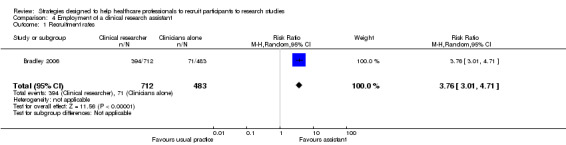
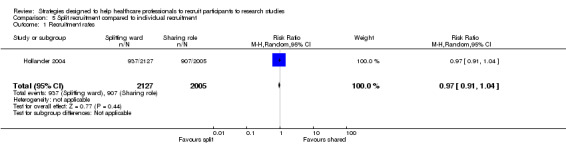
Main results: Eleven studies met our eligibility criteria and all were at medium or high risk of bias. Only five studies gave the total number of participants (totalling 7372 participants). Three studies used a randomised design, with the others using pre-post comparisons. Several different strategies were investigated. Four studies examined the impact of additional visits or information for the study site, with no increases in recruitment demonstrated. Increased recruitment rates were reported in two studies that used a dedicated clinical recruiter, and five studies that introduced an automated alert system for identifying eligible participants. The studies were embedded into trials evaluating care in oncology mainly but also in emergency departments, diabetes and lower back pain.
Authors' conclusions: There is no strong evidence for any single strategy to help healthcare professionals to recruit participants in research studies. Additional visits or information did not appear to increase recruitment by healthcare professionals. The most promising strategies appear to be those with a dedicated resource (e.g. a clinical recruiter or automated alert system) for identifying suitable participants that reduced the demand on healthcare professionals, but these were assessed in studies at high risk of bias.
Contexte: L'identification et l'approche des participants éligibles pour le recrutement dans des études de recherche repose généralement sur les professionnels de la santé. Ce processus est parfois entravé par des barrières délibérées ou accidentelles pouvant entrainer des biais dans la sélection des patients.
Objectifs: Notre principal objectif était d'identifier et d'évaluer les effets des stratégies conçues pour aider les professionnels de la santé à recruter des participants dans des études de recherche. STRATÉGIE DE RECHERCHE DOCUMENTAIRE: Nous avons effectué des recherches le 5 janvier 2015 dans les bases de données électroniques suivantes : le registre Cochrane Méthodologie, CENTRAL, MEDLINE, EMBASE, CINAHL, British Nursing Index, PsycINFO, ASSIA et Web of Science (SSCI, SCI‐EXPANDED) à partir de 1985. Nous avons examiné les références bibliographiques de toutes les études incluses et des articles de revue pertinents et nous avons suivi les références via Web of Science pour toutes les études incluses. CRITÈRES DE SÉLECTION: Nous avons sélectionné toutes les études ayant évalué une stratégie visant à identifier et à recruter des participants pour des recherches via des professionnels de la santé et ayant fourni des données de comparaison sur les taux de recrutement. RECUEIL ET ANALYSE DES DONNÉES: Deux auteurs de la revue ont indépendamment passé au crible les résultats des recherches pour évaluer l'éligibilité, lu les articles complets, appliqué les critères d'inclusion et extrait les données. Nous avons calculé les risques relatifs pour chaque étude pour déterminer l'effet de chaque stratégie. RÉSULTATS PRINCIPAUX: Onze études remplissaient nos critères d'éligibilité et celles‐ci étaient toutes à risque élevé ou modéré de biais. Seules cinq études ont indiqué le nombre total de participants (7372 participants au total). Trois études ont utilisé un plan d'étude randomisé, et les autres ont utilisé un plan de type avant/après. Plusieurs stratégies différentes ont été étudiées. Quatre études ont examiné l'impact des visites supplémentaires ou de l'offre d'informations supplémentaires aux sites des études ; aucune augmentation des taux de recrutement n'a été démontrée. Des augmentations des taux de recrutement ont été rapportées dans deux études ayant fait recours à une personne désignée s'occupant spécifiquement du recrutement, et dans cinq études ayant introduit un système d'alarme pour l'identification des participants éligibles. Les études étaient intégrées à des essais évaluant principalement des soins en oncologie mais également des services d'urgences, le diabète et les dorsalgies.
Conclusions des auteurs: Il n'existe pas de preuves solides pour appuyer une quelconque stratégie visant à aider les professionnels de la santé à recruter des participants dans des études de recherche. Des visites supplémentaires ou l'offre d'informations supplémentaires n'ont pas semblé augmenter le recrutement par les professionnels de la santé. Les stratégies les plus prometteuses semblent être celles faisant recours à une personne désignée (par exemple un recruteur pour essais cliniques ou un système d'alerte automatisé) s'occupant spécifiquement de l'identification des potentiels participants ayant réduit les pressions exercées sur les professionnels de la santé, mais celles‐ci ont été évaluées dans des études à risque élevé de biais.
Antecedentes: La identificación y el primer contacto con los participantes aptos para el reclutamiento en los estudios de investigación suele depender de los profesionales sanitarios. En ocasiones, este proceso se ve obstaculizado por un control deliberado o inadvertido que puede introducir sesgo en la selección de los pacientes.
Objetivos: El objetivo principal fue identificar y evaluar el efecto de las estrategias diseñadas para ayudar a los profesionales sanitarios a reclutar participantes para los estudios de investigación. MÉTODOS DE BÚSQUEDA: El 5 de enero de 2015 se realizaron búsquedas en las siguientes bases de datos electrónicas: Registro del Grupo Cochrane de Metodología (Cochrane Methodology Register), CENTRAL, MEDLINE, EMBASE, CINAHL, British Nursing Index, PsycINFO, ASSIA y Web of Science (SSCI, SCI‐EXPANDED) desde 1985 en adelante. Se verificaron las listas de referencias de todos los estudios incluidos y los artículos de revisión pertinentes y se realizó un rastreo de citas a través de Web of Science para todos los estudios incluidos. CRITERIOS DE SELECCIÓN: Se seleccionaron todos los estudios que evaluaron una estrategia para identificar y reclutar participantes para estudios de investigación a través de profesionales sanitarios y proporcionaron datos de comparación antes y después sobre las tasas de reclutamiento. OBTENCIÓN Y ANÁLISIS DE LOS DATOS: Dos autores de la revisión de forma independiente examinaron los resultados de la búsqueda para determinar la posible elegibilidad, leyeron los artículos completos, aplicaron los criterios de selección y extrajeron los datos. Se calcularon las razones de riesgos de cada estudio para indicar el efecto de cada estrategia.
Resultados principales: Once estudios cumplieron los criterios de elegibilidad y todos tuvieron riesgo de sesgo medio o alto. Solo cinco estudios proporcionaron el número total de participantes (en total 7372 participantes). Tres estudios utilizaron un diseño aleatorizado y los demás utilizaron comparaciones antes y después. Se investigaron varias estrategias diferentes. Cuatro estudios examinaron la repercusión de las visitas o la información adicionales para el centro de estudio, sin que se demostrara un aumento del reclutamiento. Se informó un aumento de las tasas de reclutamiento en dos estudios que utilizaron un reclutador clínico especializado, y en cinco estudios que introdujeron un sistema de alerta automatizado para identificar a los participantes elegibles. Los estudios se integraron en ensayos que evaluaron principalmente la atención en oncología, pero también en servicios de urgencias, diabetes y lumbalgia.
Conclusiones de los autores: No hay evidencia sólida de que una sola estrategia ayude a los profesionales sanitarios a reclutar participantes en los estudios de investigación. Las visitas o la información adicionales no parecieron aumentar el reclutamiento por parte de los profesionales sanitarios. Las estrategias más prometedoras parecen ser las que cuentan con un recurso dedicado (p.ej., un reclutador clínico o un sistema de alerta automatizado) para identificar a los participantes adecuados y reducir la demanda de profesionales sanitarios, pero se evaluaron en estudios con alto riesgo de sesgo.
پیشینه: شناسایی و انتخاب شرکتکنندگان واجد شرایط برای ورود در مطالعات تحقیقاتی، معمولا متکی است بر نظر متخصصان مراقبت سلامت. این فرآیند گاهی در اثر کنترل عمدی یا غیر‐عمدی که میتواند باعث سوگیری (bias) در انتخاب بیمار شود، مختل میشود. اهداف: هدف اصلی ما، شناسایی و ارزیابی تاثیر استراتژیهای طراحیشده برای کمک به متخصصان مراقبت سلامت در جذب شرکتکنندگان در مطالعات پژوهشی بود. روشهای جستوجو: جستوجوهای خود را در 5 ژانویه 2015 در بانکهای اطلاعاتی الکترونیکی زیر انجام دادیم: پایگاه ثبت متدولوژی در کاکرین (Cochrane Methodology Register)؛ CENTRAL؛ MEDLINE؛ EMBASE؛ CINAHL؛ British Nursing Index؛ PsycINFO؛ ASSIA و (Web of Science (SSCI, SCI‐EXPANDED از 1985 به بعد. همچنین فهرست منابع تمام مطالعات وارد شده و مقالات مطالعات مروری مرتبط را بررسی کرده و برای همه مطالعات وارد شده ردیابی استنادات را از طریق Web of Science انجام دادیم. معیارهای انتخاب: تمام مطالعاتی را انتخاب کردیم که به بررسی یک استراتژی برای شناسایی و جذب شرکتکنندگان در پژوهش از طریق متخصصان مراقبت سلامت پرداخته و دادههای مربوط به مقایسه قبل و بعد را درباره نرخ جذب شرکتکنندگان فراهم کردند. گردآوری و تجزیهوتحلیل دادهها: دو نویسنده مرور بهطور مستقل از هم نتایج جستوجو را از نظر واجد شرایط بودن بالقوه غربالگری کرده، متن کامل مقالات را خوانده، معیارهای انتخاب را اعمال کرده و دادهها را استخراج کردند. به منظور نشان دادن تاثیر هر استراتژی، خطر نسبی (RR) را برای هر مطالعه محاسبه کردیم. نتایج اصلی: یازده مطالعه معیارهای ورود را داشته و همگی در معرض خطر سوگیری بالا یا متوسط قرار داشتند. فقط پنج مطالعه، تعداد کل شرکتکنندگان خود را اعلام کردند (در مجموع 7372 شرکتکننده). سه مطالعه از طراحی تصادفیسازی، و بقیه از مقایسههای قبل‐بعد استفاده کردند. چندین استراتژی متفاوت بررسی شدند. چهار مطالعه تاثیر ویزیتها یا اطلاعات بیشتر را در مورد محل مطالعه بررسی کردند، اما هیچ افزایشی در میزان جذب شرکتکنندگان مشاهده نشد. در دو مطالعه که از همکاران بالینی اختصاصی و در پنج مطالعه که از سیستم هشداردهنده خودکار برای شناسایی شرکتکنندگان واجد شرایط استفاده شد، افزایش در میزان جذب شرکتکنندگان به چشم خورد. مطالعات در کارآزماییهایی تعبیه شدند که عمدتا به ارزیابی مراقبت در انکولوژی پرداختند، اما تعدادی نیز مربوط به بخشهای اورژانس، دیابت و کمردرد بودند. نتیجهگیریهای نویسندگان: شواهد قوی برای یک استراتژی واحد وجود ندارد که به متخصصان مراقبت سلامت در جذب شرکتکنندگان در مطالعات تحقیقاتی کمک کند. به نظر نمیرسید که ویزیتها یا اطلاعات بیشتر، باعث افزایش جذب شرکتکنندگان توسط متخصصان مراقبت سلامت شوند. همچنین به نظر میرسید که امیدوارکنندهترین استراتژیها مربوط به راهبردهایی با منبع اختصاصی (بهعنوان مثال استفاده از همکاران بالینی یا سیستم هشدار خودکار) برای شناسایی مناسب شرکتکنندگان بود که تقاضا را برای متخصصان مراقبت سلامت کاهش داد، اما این موضوع در مطالعاتی با خطر بالای سوگیری ارزیابی شدند.
Copyright © 2016 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
NP, CW, MF, GE, CS, CT, JH, LC, SB and CBW state there are no declarations of interest.
Figures
Update of
References
References to studies included in this review
Bell‐Syer 2000 {published data only}
-
- Bell‐Syer SE, Moffett JA. Recruiting patients to randomized trials in primary care: principles and case study. Family Practice 2000;17(2):187‐91. - PubMed
Bradley 2006 {published data only}
-
- Bradley N, Chow E, Tsao M, Danjoux C, Barnes EA, Hayter C, et al. Reasons for poor accrual in palliative radiation therapy research studies. Supportive Cancer Therapy 2006;3(2):110‐9. - PubMed
Cardozo 2010 {published data only}
-
- Cardozo E, Meurer WJ, Smith BL, Holschen JC. Utility of an automated notification system for recruitment of research subjects. Emergency Medicine Journal 2010;27:786‐7. - PubMed
Chen 2013 {published data only}
Cox 2005 {published data only}
-
- Cox K, Avis M, Wilson, E, Elkan R. An evaluation of the introduction of Clinical Trial Officer roles into the cancer clinical trial setting in the UK. European Journal of Cancer Care 2005;14:448‐56. - PubMed
Embi 2005 {published data only}
Hollander 2004 {published data only}
-
- Hollander JE, Sparano DM, Karounos M, Sites FD, Shofer FS. Studies in emergency department data collection: shared versus split responsibility for patient enrollment. Academic and Emergency Medicine 2004;11(2):200‐3. - PubMed
Kimmick 2005 {published data only}
-
- Kimmick GG, Peterson BL, Kornblith AB, Mandelblatt J, Johnson JL, Wheeler J, et al. Improving accrual of older persons to cancer treatment trials: a randomized trial comparing an educational intervention with standard information. Journal of Clinical Oncology 2005;23(10):2201‐7. - PubMed
Lienard 2006 {published data only}
-
- Lienard JL, Quinaux E, Fabre‐Guillevin E, Piedbois P, Jouhsuf A, Decoster G, et al on behalf of the European Association. Impact of on‐site initiation visits on patient recruitment and data quality in a randomized trial of adjuvant chemotherapy for breast cancer. Clinical Trials 2006;3:486‐92. - PubMed
Monaghan 2007 {published data only}
-
- Monaghan H, Richens A, Colman S, Currie R, Girgis S, Jayne K, et al. A randomised trial of the effects of an additional communication strategy on recruitment into a large‐scale, multi‐centre trial. Contemporary Clinical Trials 2007;28:1‐5. - PubMed
Paskett 2002 {published data only}
-
- Paskett ED, Cooper MR, Stark N, Ricketts TC, Tropman S, Hatzell T, et al. Clinical trial enrollment of rural patients with cancer. Cancer Practice 2002;10(1):28‐35. - PubMed
Additional references
Barnes 2005
-
- Barnes S, Gott M, Payne S, Parker C, Seamark D, Gariballa S, et al. Recruiting older people into a large, community‐based study of heart failure. Chronic Illness 2005;1:321‐9. - PubMed
Bryant 2005
Darbyshire 2011
-
- Darbyshire J, Sitzia J, Cameron D, Ford G, Littlewood S, Kaplan R, et al. Extending the clinical research network approach to all of healthcare. Annals of Oncology 2011;22(Suppl 7):vii36‐43. - PubMed
Data Protection Act 1998
-
- UK Parliament. Data Protection Act. HMSO, London 1998.
Department of Health 2009
-
- Department of Health. Requirements to support research in the NHS. Department of Health, London 2009.
Ewing 2004
-
- Ewing G, Rogers M, Barclay S, McCabe J, Martin A, Todd C. Recruiting patients into a primary care based study of palliative care: why is it so difficult?. Palliative Medicine 2004;18:452‐9. - PubMed
Higgins 2011
-
- Higgins J, Altman D. Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Horsley 2011
Ives 2009
-
- Ives J, Draper H, Damery S, Wilson S. Do family doctors have an obligation to facilitate research?. Family Practice 2009;26:543‐8. - PubMed
Lawlor 2001
-
- Lawlor DA, Stone T. Public health and data protection: an inevitable collision or potential for a meeting of minds?. International Journal of Epidemiology 2001;30:1221‐5. - PubMed
Lewis 2001
Mason 2007
-
- Mason VL, Shaw A, Wiles NJ, Mulligan J, Peters TJ, Sharp D, et al. GPs' experiences of primary care mental health research: a qualitative study of the barriers to recruitment. Family Practice 2007;24:518‐25. - PubMed
McDonald 2006
Pocock 2008
-
- Pocock SJ. The size of a clinical trial. Clinical Trials: A Practical Approach. Chichester: John Wiley & Sons, 2008.
Redsell 1998
-
- Redsell SA, Cheater FM. The Data Protection Act (1998): implications for health researchers. Journal of Advanced Nursing 2001;35:508‐13. - PubMed
Rendell 2007
Salman 2014
Smith 2013
-
- Smith V, Clarke M, Devane D, Begley C, Shorter G, Maguire L. SWAT 1: What effects do site visits by the principal investigator have on recruitment in a multicentre randomized trial?. Journal of Evidence‐based Medicine 2013;6(3):136‐7. [PUBMED: 24325369] - PubMed
Smith 2015
Stratford 1998
-
- Stratford JS, Stratford J. Data protection and privacy in the United States and Europe. International Association for Social Science Information Services and Technology 1998;Fall:17‐20.
Strobl 2000
Treweek 2010
White 2008
-
- White C, Hardy J. Gatekeeping from palliative care research trials. Progress in Palliative Care 2008;16:167‐71.
References to other published versions of this review
Preston 2012
-
- Preston NJ, Farquhar MC, Walshe CE, Stevinson C, Ewing G, Calman LA, Burden S, Brown Wilson C, Hopkinson JB, Todd C. Strategies to increase participant recruitment to research studies by healthcare professionals. Cochrane Database of Systematic Reviews 2012, Issue 9. [DOI: 10.1002/14651858.MR000036] - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous