

Treatment for inclusion body myositis
- PMID: 35658164
- PMCID: PMC9645777
- DOI: 10.1002/14651858.CD001555.pub5
Treatment for inclusion body myositis
Abstract
Background: Inclusion body myositis (IBM) is a late-onset inflammatory muscle disease (myopathy) associated with progressive proximal and distal limb muscle atrophy and weakness. Treatment options have attempted to target inflammatory and atrophic features of this condition (for example with immunosuppressive and immunomodulating drugs, anabolic steroids, and antioxidant treatments), although as yet there is no known effective treatment for reversing or minimising the progression of inclusion body myositis. In this review we have considered the benefits, adverse effects, and costs of treatment in targeting cardinal effects of the condition, namely muscle atrophy, weakness, and functional impairment.
Objectives: To assess the effects of treatment for IBM.
Search methods: On 7 October 2014 we searched the Cochrane Neuromuscular Disease Group Specialized Register, the Cochrane Central Register for Controlled Trials (CENTRAL), MEDLINE, and EMBASE. Additionally in November 2014 we searched clinical trials registries for ongoing or completed but unpublished trials.
Selection criteria: We considered randomised or quasi-randomised trials, including cross-over trials, of treatment for IBM in adults compared to placebo or any other treatment for inclusion in the review. We specifically excluded people with familial IBM and hereditary inclusion body myopathy, but we included people who had connective tissue and autoimmune diseases associated with IBM, which may or may not be identified in trials. We did not include studies of exercise therapy or dysphagia management, which are topics of other Cochrane systematic reviews.
Data collection and analysis: We used standard Cochrane methodological procedures.
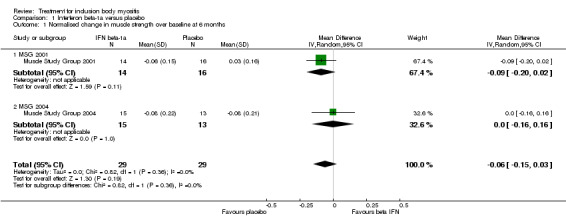
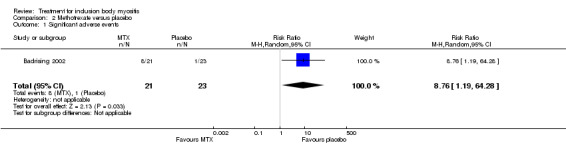
Main results: The review included 10 trials (249 participants) using different treatment regimens. Seven of the 10 trials assessed single agents, and 3 assessed combined agents. Many of the studies did not present adequate data for the reporting of the primary outcome of the review, which was the percentage change in muscle strength score at six months. Pooled data from two trials of interferon beta-1a (n = 58) identified no important difference in normalised manual muscle strength sum scores from baseline to six months (mean difference (MD) -0.06, 95% CI -0.15 to 0.03) between IFN beta-1a and placebo (moderate-quality evidence). A single trial of methotrexate (MTX) (n = 44) provided moderate-quality evidence that MTX did not arrest or slow disease progression, based on reported percentage change in manual muscle strength sum scores at 12 months. None of the fully published trials were adequately powered to detect a treatment effect. We assessed six of the nine fully published trials as providing very low-quality evidence in relation to the primary outcome measure. Three trials (n = 78) compared intravenous immunoglobulin (combined in one trial with prednisone) to a placebo, but we were unable to perform meta-analysis because of variations in study analysis and presentation of trial data, with no access to the primary data for re-analysis. Other comparisons were also reported in single trials. An open trial of anti-T lymphocyte immunoglobulin (ATG) combined with MTX versus MTX provided very low-quality evidence in favour of the combined therapy, based on percentage change in quantitative muscle strength sum scores at 12 months (MD 12.50%, 95% CI 2.43 to 22.57). Data from trials of oxandrolone versus placebo, azathioprine (AZA) combined with MTX versus MTX, and arimoclomol versus placebo did not allow us to report either normalised or percentage change in muscle strength sum scores. A complete analysis of the effects of arimoclomol is pending data publication. Studies of simvastatin and bimagrumab (BYM338) are ongoing. All analysed trials reported adverse events. Only 1 of the 10 trials interpreted these for statistical significance. None of the trials included prespecified criteria for significant adverse events.
Authors' conclusions: Trials of interferon beta-1a and MTX provided moderate-quality evidence of having no effect on the progression of IBM. Overall trial design limitations including risk of bias, low numbers of participants, and short duration make it difficult to say whether or not any of the drug treatments included in this review were effective. An open trial of ATG combined with MTX versus MTX provided very low-quality evidence in favour of the combined therapy based on the percentage change data given. We were unable to draw conclusions from trials of IVIg, oxandrolone, and AZA plus MTX versus MTX. We need more randomised controlled trials that are larger, of longer duration, and that use fully validated, standardised, and responsive outcome measures.
Antecedentes: La miositis por cuerpos de inclusión (MCI) es una enfermedad muscular inflamatoria (miopatía) de aparición tardía asociada con atrofia muscular y debilidad progresivas de los miembros proximales y distales. Las opciones de tratamiento se han intentado dirigir a las características inflamatorias y atróficas de esta afección (por ejemplo, con fármacos inmunosupresores e inmunomoduladores, esteroides anabólicos y tratamientos antioxidantes), aunque hasta ahora no hay un tratamiento eficaz conocido para la reversión o la reducción de la progresión de la miositis por cuerpos de inclusión. En esta revisión se han considerado los efectos beneficiosos, los efectos adversos y los costos del tratamiento dirigido a los efectos fundamentales de la afección, a saber, la atrofia muscular, la debilidad y el deterioro funcional.
Objetivos: Evaluar los efectos del tratamiento para la MCI. MÉTODOS DE BÚSQUEDA: El 7 octubre 2014, se hicieron búsquedas en el registro especializado del Grupo Cochrane de Enfermedades Neuromusculares (Cochrane Neuromuscular Disease Group), en el Registro Cochrane Central de Ensayos Controlados (Cochrane Central Register of Controlled Trials) (CENTRAL), MEDLINE y en EMBASE. Además, en noviembre 2014 se realizaron búsquedas de ensayos en curso o terminadas pero no publicados en los registros de ensayos clínicos. CRITERIOS DE SELECCIÓN: Se consideraron para inclusión en la revisión los ensayos aleatorios o cuasialeatorios, incluidos los ensayos cruzados (crossover), del tratamiento para la MCI en adultos en comparación con placebo u otro tratamiento. Se excluyeron específicamente los pacientes con MCI familiar y miopatía por cuerpos de inclusión hereditaria, pero se incluyeron los pacientes con enfermedades del tejido conjuntivo y autoinmunitarias asociadas con MCI, que pueden o no identificarse en los ensayos. No se incluyeron los estudios de terapia con ejercicios o tratamiento de la disfagia, que son los temas de otras revisiones sistemáticas Cochrane. OBTENCIÓN Y ANÁLISIS DE LOS DATOS: Se utilizaron procedimientos metodológicos Cochrane estándar.
Resultados principales: La revisión incluyó diez ensayos (249 participantes) que utilizaron diferentes regímenes de tratamiento. Siete de los diez ensayos evaluaron agentes únicos y tres evaluaron agentes combinados. Muchos de los estudios no presentaron datos suficientes para el informe del resultado primario de la revisión, que fue el cambio porcentual en la puntuación de fuerza muscular a los seis meses. Los datos agrupados de dos ensayos de interferón beta‐1a (n = 58) no identificaron diferencias importantes en las puntuaciones normalizadas de la suma de la fuerza muscular manual desde el inicio hasta los seis meses (diferencia de medias [DM] ‐0,06; IC del 95%: ‐0,15 a 0,03) entre IFN beta‐1a y placebo (pruebas de calidad moderada). Un único ensayo de metotrexato (MTX) (n = 44) proporcionó pruebas de calidad moderada de que el MTX no detuvo ni enlenteció la progresión de la enfermedad, sobre la base del cambio porcentual informado en las puntuaciones de la suma de la fuerza muscular manual a los 12 meses. Ninguno de los ensayos publicados completamente tuvo poder estadístico suficiente para detectar un efecto del tratamiento. Se consideró que seis de los nueve ensayos publicados completamente aportaron pruebas de calidad muy baja con respecto a la medida de resultado primaria. Tres ensayos (n = 78) compararon la inmunoglobulina intravenosa (combinada en un ensayo con prednisona) con placebo, pero no fue posible realizar el metanálisis debido a las variaciones en el análisis de los estudios y a la presentación de los datos del ensayo, sin acceso a los datos primarios para el reanálisis. Otras comparaciones también se informaron en ensayos individuales. Un ensayo abierto de inmunoglobulina anti‐linfocitos T (IgAT) combinada con MTX versus MTX proporcionó pruebas de calidad muy baja a favor del tratamiento combinado, sobre la base del cambio porcentual en las puntuaciones cuantitativas de la suma de la fuerza muscular a los 12 meses (DM 12,50%; IC del 95%: 2,43 a 22,57). Los datos de los ensayos de oxandrolona versus placebo, azatioprina (AZA) combinada con MTX versus MTX y arimoclomol versus placebo no permitieron informar sobre el cambio porcentual o normalizado en las puntuaciones de la suma de la fuerza muscular. Un análisis completo de los efectos del arimoclomol está pendiente de la publicación de los datos. Están en curso estudios de simvastatina y bimagrumab (BYM338). Todos los ensayos analizados informaron eventos adversos. Solamente uno de los diez ensayos interpretó la significación estadística de los eventos adversos. Ninguno de los ensayos incluyó criterios preespecificados para los eventos adversos significativos.
Conclusiones de los autores: Los ensayos de interferón beta‐1a y MTX proporcionaron pruebas de calidad moderada de que no tienen efectos sobre la progresión de la MCI. Las limitaciones generales del diseño de los ensayos, que incluyen el riesgo de sesgo, los escasos números de participantes y la corta duración, hacen difícil determinar si alguno de los tratamientos farmacológicos incluidos en esta revisión fue eficaz. Un ensayo abierto de ATG combinada con MTX versus MTX aportó pruebas de calidad muy baja a favor del tratamiento combinado sobre la base de los datos de cambio porcentual facilitados. No fue posible establecer conclusiones de los ensayos de IgIV, oxandrolona y AZA más MTX versus MTX. Se necesitan más ensayos controlados aleatorios de mayor tamaño, con una duración más prolongada y que utilicen medidas de resultado completamente validadas, estandarizadas y de interés.
Copyright © 2015 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
MR is a member of the Muscle Study Group that published the two trials of IFN beta‐1a for IBM. These trials were grant funded with a proportion of those funds paid to my institution for the conduct of the trial only and with no personal financial benefit ensuing. For these trials the drug (Avonex) and matching placebo were supplied free of charge by the manufacturer Biogen. The trial protocols, data entry, data analysis, and publications were in the hands of the investigators with no input from Biogen.
KJ's research contribution has been paid for by a grant from the Association Française contre les Myopathies.
KL has no known financial conflicts of interest.
MW has published one randomised trial of IVIg in IBM. She contributed to the Novartis EU Local Advisory Board Meeting (IBM BYM338 trial) on 15 April 2013.
JM has been a member of advisory boards for CSL Behring, Octapharma, and Grifols, companies that produce IVIg. He received meeting expenses to attend Peripheral Nerve Society meetings in 2011, 2012, and 2013 from Baxter and CSL Behring, which produce IVIg products. He is a local principal investigator for the RESILIENT study, an ongoing study of bimagrumab in sporadic IBM sponsored by Novartis.
MD has published three randomised trials of IVIg in IBM. He has accepted institutional grants unrelated to the present review from: CSL, Genesis, Merck, Novartis, and Genzyme. He has also received personal compensation for lectures or consultancies from Novartis, Dysimmune Diseases Foundation, Therapath, Genzyme, Octapharma, and Baxter.
RB has no known financial conflicts of interest. She is Managing Editor of the Cochrane Neuromuscular Disease Group.
RG is a member of the Muscle Study Group that published two trials of IFN beta‐1a for IBM. He has no other known conflicts of interest.
Figures





Update of
References
References to studies included in this review
Badrising 2002 {published data only}
-
- Badrising UA, Maat‐Schieman ML, Ferrari MD, Zwinderman AH, Wessels JA, Breedveld FC, et al. Comparison of weakness progression in inclusion body myositis during treatment with methotrexate or placebo. Annals of Neurology 2002;51(3):369‐72. [PUBMED: 11891832] - PubMed
Dalakas 1997 {published data only}
-
- Dalakas MC, Sonies B, Dambrosia J, Sekul E, Cupler E, Sivakumar K. Treatment of inclusion‐body myositis with IVIg: a double‐blind, placebo‐controlled study. Neurology 1997;48(3):712‐6. [PUBMED: 9065553] - PubMed
-
- Fujii M, Koffman B, Sivakumar K, Dalakas MC. Histologic characteristics in repeated muscle biopsies of patients with inclusion body myositis treated in a control trial with high‐dose intravenous immunoglobulin and prednisone. Neurology 1997;48 Suppl 2:A332‐3.
Dalakas 2001 {published data only}
-
- Dalakas MC, Koffman B, Fujii M, Spector S, Sivakumar K, Cupler E. A controlled study of intravenous immunoglobulin combined with prednisolone in the treatment of IBM. Neurology 2001;56(3):323‐7. [PUBMED: 11171896] - PubMed
Leff 1993 {published data only}
-
- Leff RL, Miller FW, Hicks J, Fraser DD, Plotz PH. The treatment of inclusion body myositis: a retrospective review and a randomised prospective trial of immunosuppressive therapy. Medicine 1993;72(4):225‐35. [PUBMED: 8393509] - PubMed
Lindberg 2003 {published data only}
-
- Lindberg C, Trysberg E, Tarkowski A, Oldfors A. Anti‐T‐lymphocyte globulin treatment in inclusion body myositis: a randomized pilot study. Neurology 2003;61(2):260‐2. [PUBMED: 12874415] - PubMed
Machado 2013 {published and unpublished data}
-
- Machado P, Miller A, Herbelin L, He J, Noel J, Wang Y, et al. Safety and tolerability of arimoclomol in patients with sporadic inclusion body myositis: a randomised, double‐blind, placebo‐controlled, phase IIA proof‐of‐concept trial. Annals of the Rheumatic Diseases 2013;72(Suppl 3):A164.
-
- Machado P, Miller A, Herbelin L, He J, Wang Y, McVey AL, et al. Arimoclomol study in IBM: [personal communication]. Email to P Machado 4 November 2014.
Muscle Study Group 2001 {published data only}
-
- The Muscle Study Group. Randomized pilot trial of betaINF1a (Avonex) in patients with inclusion body myositis. Neurology 2001;57(9):1566‐70. [PUBMED: 11706093] - PubMed
Muscle Study Group 2004 {published data only}
-
- The Muscle Study Group. Randomized pilot trial of high‐dose betaINF‐1a in patients with inclusion body myositis. Neurology 2004;63(4):718‐20. [PUBMED: 15326251] - PubMed
Rutkove 2002 {published data only}
-
- Rutkove SB, Parker RA, Nardin RA, Connolly CE, Felice KJ, Raynor EM. A pilot randomized trial of oxandrolone in inclusion body myositis. Neurology 2002;58(7):1081‐7. [PUBMED: 11940697] - PubMed
Walter 2000 {published data only}
-
- Pongratz D, Lochmuller H, Toepfer M, Schlotter B, Schroder M, Muller‐Felber W, et al. High dose intravenous immunoglobulin (IVIG) in the treatment of inclusion body myositis ‐ a double‐blind placebo‐controlled study. Muscle & Nerve 1998;21(Suppl 7):S131. - PubMed
-
- Walter MC, Lochmuller H, Toepfer M, Schlotter B, Reilich P, Schroder M, et al. High‐dose immunoglobulin therapy in sporadic inclusion body myositis: a double blind, placebo‐controlled study. Journal of Neurology 2000;247(1):22‐8. [PUBMED: 10701893] - PubMed
References to studies excluded from this review
ACTRN12614000082606 {published data only}
-
- ACTRN12614000082606. Pilot study of the treatment of patients with sporadic inclusion body myositis with the anaplerotic medication Triheptanoin. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=365625 (accessed 6 November 2014).
Amato 1994 {published data only}
-
- Amato AA, Barohn RJ, Jackson CE, Pappert EJ, Sahenk Z, Kissel JT. Inclusion body myositis: treatment with intravenous immunoglobulin. Neurology 1994;44(8):1516‐8. [PUBMED: 8058161] - PubMed
Arnardottir 2003 {published data only}
-
- Arnardottir S, Alexanderson H, Lundberg IE, Borg K. Sporadic inclusion body myositis: pilot study on the effects of a home exercise program on muscle function, histopathology and inflammatory reaction. Journal of Rehabilitation Medicine 2003;35(1):31‐5. [PUBMED: 12610846 ] - PubMed
Danon 1982 {published data only}
-
- Danon MJ, Reyes MG, Perurena OH, Masdeu JC, Manaligod JR. Inclusion body myositis. A corticosteroid‐resistant idiopathic inflammatory myopathy. Archives of Neurology 1982;39(12):760‐4. [PUBMED: 6291495] - PubMed
Heikkillä 2001 {published data only}
-
- Heikkillä S, Viitanen JV, Kautiainen H, Rajamäki T, Mäntyvuo P, Harju T. Rehabilitation in myositis: preliminary study. Physiotherapy 2001;87(6):301‐9.
Joffe 1993 {published data only}
-
- Joffe MM, Love LA, Leff RL, Fraser DD, Targoff IN, Hicks JE, et al. Drug therapy of the idiopathic inflammatory myopathies: predictors of response to prednisone, azathioprine, and methotrexate and a comparison of their efficacy. American Journal of Medicine 1993;94(4):379‐87. [PUBMED: 8386437] - PubMed
Kosmidis 2013 {published data only}
-
- Kosmidis ML, Alexopoulos H, Tzioufas AG, Dalakas MC. The effect of anakinra, an IL1 receptor antagonist, in patients with sporadic inclusion body myositis (sIBM): a small pilot study. Journal of the Neurological Sciences 2013;334(1‐2):1235. - PubMed
-
- NCT01165008. Anakinra in myositis. http://www.clinicaltrials.gov/ct2/show/NCT01165008 (accessed 6 November 2014).
Lindberg 1994 {published data only}
-
- Lindberg C, Persson LI, Bjorkander J, Oldfors A. Inclusion body myositis: clinical, morphological, physiological and laboratory findings in 18 cases. Acta Neurologica Scandinavica 1994;89(2):123‐31. [PUBMED: 8191875] - PubMed
Mastaglia 1998 {published data only}
Mowzoon 2001 {published data only}
-
- Mowzoon N, Sussman A, Bradley WG. Mycophenolate (CellCept) treatment of myasthenia gravis, chronic inflammatory polyneuropathy and inclusion body myositis. Journal of the Neurological Sciences 2001;185(2):119‐22. [PUBMED: 11311292] - PubMed
NCT00079768 {published data only}
-
- NCT00079768. Alemtuzumab to treat sporadic inclusion body myositis. http://www.clinicaltrials.gov/ct2/show/NCT00079768 (accessed 6 November 2014).
NCT00917956 {published data only}
-
- NCT00917956. Lithium in inclusion body myositis (IBM) (Li‐IBM). http://www.clinicaltrials.gov/ct2/show/NCT00917956 (accessed 6 November 2014).
NCT01519349 {published data only}
-
- NCT01519349. Follistatin gene transfer to patients with Becker muscular dystrophy and sporadic inclusion body myositis. http://www.clinicaltrials.gov/ct2/show/NCT01519349 (accessed 6 November 2014).
Soueidan 1993 {published data only}
-
- Soueidan SA, Dalakas M. Treatment of inclusion‐body myositis with high‐dose intravenous immunoglobulin. Neurology 1993;43(5):876‐9. [PUBMED: 8492940] - PubMed
References to ongoing studies
EUCTR2007‐004359‐12‐IT {published data only}
-
- EUCTR2007‐004359‐12‐IT. Simvastatin treatment in inclusion body myositis (IBM) ‐ ND. http://apps.who.int/trialsearch/Trial.aspx?TrialID=EUCTR2007‐004359‐12‐IT (accessed 6 November 2014). [EUCTR2007‐004359‐12‐IT]
NCT00001265 {published data only}
-
- NCT00001265. Study and treatment of inflammatory muscle diseases. http://www.clinicaltrials.gov/show/NCT00001265 (accessed 6 November 2014).
NCT01423110 {published data only}
-
- NCT01423110. Efficacy and safety of bimagrumab/BYM338 at 52 weeks on physical function, muscle strength, mobility in sIBM patients. http://www.clinicaltrials.gov/ct2/show/NCT01423110 (accessed 6 November 2014).
-
- NCT01423110. Efficacy, safety and tolerability of BYM338 in patients with sporadic inclusion body myositis. http://www.clinicaltrials.gov/ct2/show/NCT01423110 (accessed 6 November 2014).
-
- NCT02250443. Study of long‐term safety, efficacy tolerability of BYM338 in patients with sporadic inclusion body myositis. http://www.clinicaltrials.gov/ct2/show/NCT02250443 (accessed 6 November 2014).
Additional references
Amato 1998
-
- Amato AA, Shebert RT. Inclusion body myositis in twins. Neurology 1998;51(2):598‐600. - PubMed
Aronson 2006
-
- Aronson JK (editor). Meyler's Side Effects of Drugs: The International Encyclopedia of Adverse Drug Reactions and Interactions. Meyler's Side Effects of Drugs: The International Encyclopedia of Adverse Drug Reactions and Interactions. 15th Edition. Amsterdam: Elsevier BV, 2006.
Badrising 2000
-
- Badrising UA, Maat‐Schieman M, Duinen SG, Breedveld F, Doorn P, Engelen B, et al. Epidemiology of inclusion body myositis in the Netherlands: a nationwide study. Neurology 2000;55(9):1385‐8. - PubMed
Beaston‐Blaakman 2007
-
- Beaston‐Blaakman A, Shepard DS, Stone N, Shevitz AH. Cost‐effectiveness of clinical interventions for AIDS wasting. AIDS Care 2007;19(8):996‐1001. - PubMed
Benveniste 2010
-
- Benveniste O, Hilton‐Jones D. International Workshop on Inclusion Body Myositis held at the Institute of Myology, Paris, on 29 May 2009. Neuromuscular Disorders 2010;20(6):414‐21. - PubMed
Benveniste 2011
-
- Benveniste O, Guiget M, Freebody J, Dubourg O, Squier W, Maisonobe T, et al. Long‐term observational study of sporadic inclusion body myositis. Brain 2011;134(Pt 1):3176‐84. - PubMed
BNF 2014
-
- Joint Formulary Committee. British National Formulary. Vol. 68, London: British Medical Association and Royal Pharmaceutical Society of Great Britain, 2014.
Bohan 1975
-
- Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts). The New England Journal of Medicine 1975;292(7):344‐7. [PUBMED: 1090839] - PubMed
Breithaupt 2013
-
- Breithaupt M, Schmidt J. Update on treatment of inclusion body myositis. Current Rheumatology Reports 2013;15(5):329. - PubMed
Brooke 1983
-
- Brooke MH, Fenichel GM, Griggs RC, Mendell JR, Moxley R, Miller JP, et al. Clinical investigation in Duchenne dystrophy 2: determination of the "power" of therapeutic trials based on the natural history. Muscle & Nerve 1983;6(2):91‐103. [PUBMED: 6343858] - PubMed
Chalker 2000
-
- Chalker J, Leuwer M, Lunde PKM, McInnes GT, Thelle D, Velo GP, et al. Meyler's Side Effects of Drugs. 14th Edition. Amsterdam: Elsevier Science B.V., 2000.
Cochrane 2015
-
- The Cochrane Collaboration. Cochrane glossary. http://www.cochrane.org/glossary (accessed 27 January 2015).
Convery 1977
-
- Convery FR, Minteer MA, Amiel D, Connett KL. Polyarticular disability: a functional assessment. Archives of Physical Medicine and Rehabilitation 1977;58(11):494‐9. - PubMed
Cortese 2013
-
- Cortese A, Machado P, Morrow J, Dewar L, Hiscock A, Miller A, et al. Longitudinal observational study of sporadic inclusion body myositis: implications for clinical trials. Neuromuscular Disorders 2013;23(5):404‐12. - PubMed
Cox 2011
-
- Cox FM, Titulaer MJ, Sont JK, Wintzen AR, Verschuuren JJ, Badrising UA. A 12‐year follow‐up in sporadic inclusion body myositis: an end stage with major disabilities. Brain 2011;134(Pt 11):3167‐75. - PubMed
Dalakas 1993
-
- Dalakas MC, Illa I, Dambrosia JM, Soueidan SA, Stein DP, Otero C, et al. A controlled trial of high‐dose intravenous immunoglobulin infusions as treatment for dermatomyositis. The New England Journal of Medicine 1993;329(27):1993‐2000. [PUBMED: 8247075] - PubMed
Dalakas 1995
-
- Dalakas MC, Illa I. Common variable immunodeficiency and inclusion body myositis ‐ a distinct myopathy mediated by natural killer cells. Annals of Neurology 1995;37(6):806‐10. - PubMed
Danon 1986
-
- Danon MJ, Perurena OH, Ronan S, Manaligod JR. Inclusion body myositis associated with systemic sarcoidosis. Canadian Journal of Neurological Sciences 1986;13(4):334‐6. - PubMed
DH 2011
-
- Department of Health. Clinical guidelines for immunoglobulin use: update to second edition. http://www.ivig.nhs.uk/documents/dh_129666.pdf (accessed 27 January 2015) 2011.
Dukes 2000
-
- Dukes MNG, Aaronson JK. Meyler's Side Effects of Drugs. 14th Edition. Oxford: Elsevier, 2000.
Dutch GBS 1994
-
- Dutch Guillain‐Barre Syndrome Study Group. Treatment of Guillain‐Barre syndrome with high‐dose immune globulins combined with methylprednisolone: a pilot study. Annals of Neurology 1994;35(6):749‐52. [PUBMED: 8210234] - PubMed
Elbourne 2002
-
- Elbourne DR, Altman DG, Higgins JP, Curtin F, Worthington HV, Vail A. Meta‐analyses involving cross‐over trials: methodological issues. International Journal of Epidemiology 2002;31(1):140‐9. - PubMed
Fergusson 2005
-
- Fergusson D, Hutton B, Sharma M, Tinmouth A, Wilson K, Cameron DW, et al. Use of intravenous immunoglobulin for treatment of neurologic conditions: a systematic review. Transfusion 2005;45(10):1640‐57. - PubMed
GRADEpro 2014 [Computer program]
-
- McMaster University. GRADEpro. Hamilton, Ontario: McMaster University, 2014. www.gradepro.org.
Griggs 1995
-
- Griggs RC, Askanas V, DiMauro S, Engel A, Karpati G, Mendell JR, et al. Inclusion body myositis and myopathies. Annals of Neurology 1995;38(5):705‐13. [PUBMED: 7486861] - PubMed
Gutmann 1985
-
- Gutmann L, Govindan S, Riggs JE, Schochet SSJ. Inclusion body myositis and Sjogren's syndrome. Archives of Neurology 1985;42(10):1021‐2. - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hill 2004
Hilton‐Jones 2010
-
- Hilton‐Jones D, Miller A, Parton M, Holton J, Sewry C, Hanna MG. Inclusion body myositis: MRC Centre for Neuromuscular Diseases, IBM workshop, London, 13 June 2008. Neuromuscular Disorders 2010;20(2):142‐7. - PubMed
Huizing 2009
Jackson 2008
-
- Jackson CE, Barohn RJ, Gronseth G, Pandya S, Herbelin L. Inclusion body myositis functional rating scale: a reliable and valid measure of disease severity. Muscle & Nerve 2008;37(4):473–6. - PubMed
Khraishi 1992
-
- Khraishi MM, Jay V, Keystone EC. Inclusion body myositis in association with vitamin B12 deficiency and Sjögren's syndrome. Journal of Rheumatology 1992;19(2):306‐9. - PubMed
Lane 1985
Lindberg 1990
-
- Lindberg C, Persson L, Oldfors A, Soderstrom T, Hedstrom A, Bjorkander J. Inclusion body myositis: association with immunodeficiency. Journal of the Neurological Sciences 1990;98 (Suppl):178.
Loke 2007
Lotz 1989
-
- Lotz BP, Engel AG, Nishino H, Stevens JC, Litchy WJ. Inclusion body myositis. Observations in 40 patients. Brain 1989;112(Pt 3):727‐47. [PUBMED: 2543478] - PubMed
Machado 2013b
Needham 2008
-
- Needham M, Corbett A, Day T, Christiansen F, Fabian V, Mastaglia F. Prevalence of sporadic inclusion body myositis and factors contributing to delayed diagnosis. Journal of Clinical Neuroscience 2008;15(12):1350‐3. - PubMed
Oldfors 1995
-
- Oldfors A, Moslemi AR, Fyhr IM, Holme E, Larsson NG, Lindberg C. Mitochondrial DNA deletions in muscle fibers in inclusion body myositis. Journal of Neuropathology & Experimental Neurology 1995;54(4):581‐7. - PubMed
Pfeffer 2012
Phillips 2000
-
- Phillips BA, Zilko PJ, Mastaglia FL. Prevalence of sporadic inclusion body myositis in Western Australia. Muscle & Nerve 2000;23(6):970‐2. - PubMed
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Riggs 1984
-
- Riggs JE, Schochet SSJ, Gutmann L, McComas CF, Rogers JS. Inclusion body myositis and chronic immune thrombocytopenia. Archives of Neurology 1984;41(1):93‐5. - PubMed
Rose 2001
-
- Rose MR, McDermott MP, Thornton CA, Palenski C, Martens WB, Griggs RC. A prospective natural history study of inclusion body myositis: implications for clinical trials. Neurology 2001;57(3):548‐50. [PUBMED: 11502935] - PubMed
Rygiel 2014
Santorelli 1996
-
- Santorelli FM, Sciacco M, Tanji K, Shanske S, Vu TH, Golzi V, et al. Multiple mitochondrial DNA deletions in sporadic inclusion body myositis: a study of 56 patients. Annals of Neurology 1996;39(6):789‐95. - PubMed
Smith 2012
Soden 1994
-
- Soden M, Boundy K, Burrow D, Blumbergs P, Ahern M. Inclusion body myositis in association with rheumatoid arthritis. Journal of Rheumatology 1994;21:344‐6. - PubMed
Tateyama 2003
-
- Tateyama M, Saito N, Fujihara K, Shiga Y, Takeda A, Narikawa K, et al. Familial inclusion body myositis: a report on two Japanese sisters. Internal Medicine (Tokyo, Japan) 2003;42(10):1035‐8. - PubMed
Verschuuren 1997
-
- Verschuuren JJ, Badrising UA, Wintzen AR, Engelen BGM, Hoeven H, et al. Inclusion body myositis. In: Emery AEH editor(s). Diagnostic Criteria for Neuromuscular Disorders. London: Royal Society of Medicine Press, 1997:81–4.
Voet 2013
-
- Voet NBM, Kooi EL, Riphagen II, Lindeman E, Engelen BGM, Geurts ACH. Strength training and aerobic exercise training for muscle disease. Cochrane Database of Systematic Reviews 2013, Issue 7. [DOI: 10.1002/14651858.CD003907.pub4] - DOI