

Amitriptyline for fibromyalgia in adults
- PMID: 35658166
- PMCID: PMC6485478
- DOI: 10.1002/14651858.CD011824
Amitriptyline for fibromyalgia in adults
Abstract
Background: This is an updated version of the original Cochrane review published in Issue 12, 2012. That review considered both fibromyalgia and neuropathic pain, but the efficacy of amitriptyline for neuropathic pain is now dealt with in a separate review. Amitriptyline is a tricyclic antidepressant that is widely used to treat fibromyalgia, and is recommended in many guidelines. It is usually used at doses below those at which the drugs act as antidepressants.
Objectives: To assess the analgesic efficacy of amitriptyline for relief of fibromyalgia, and the adverse events associated with its use in clinical trials.
Search methods: We searched CENTRAL, MEDLINE, and EMBASE to March 2015, together with reference lists of retrieved papers, previous systematic reviews and other reviews, and two clinical trial registries. We also used our own hand searched database for older studies.
Selection criteria: We included randomised, double-blind studies of at least four weeks' duration comparing amitriptyline with placebo or another active treatment in fibromyalgia.
Data collection and analysis: We extracted efficacy and adverse event data, and two study authors examined issues of study quality independently. We performed analysis using three tiers of evidence. First tier evidence derived from data meeting current best standards and subject to minimal risk of bias (outcome equivalent to substantial pain intensity reduction, intention-to-treat analysis without imputation for dropouts; at least 200 participants in the comparison, 8 to 12 weeks duration, parallel design), second tier from data that failed to meet one or more of these criteria and were considered at some risk of bias but with adequate numbers in the comparison, and third tier from data involving small numbers of participants that were considered very likely to be biased or used outcomes of limited clinical utility, or both. For efficacy, we calculated the number needed to treat to benefit (NNT), and for harm we calculated the number needed to treat to harm (NNH) for adverse events and withdrawals. We used a fixed-effect model for meta-analysis.
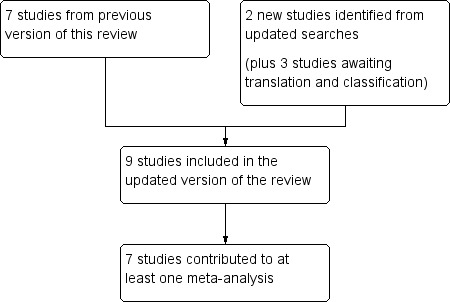
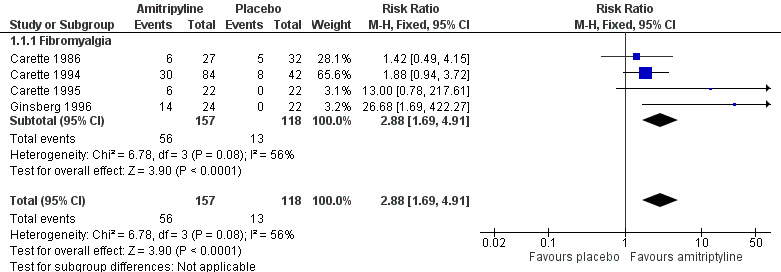
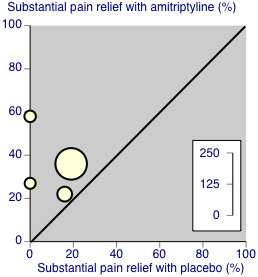
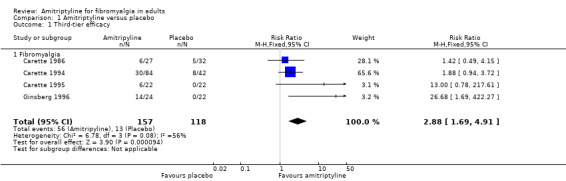
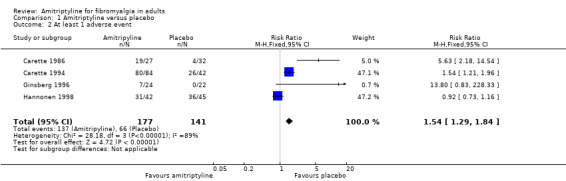
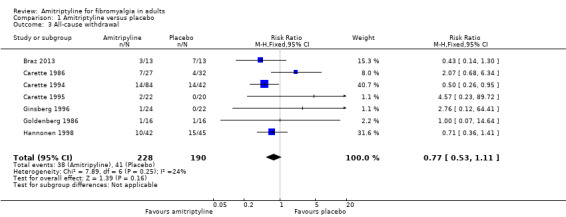
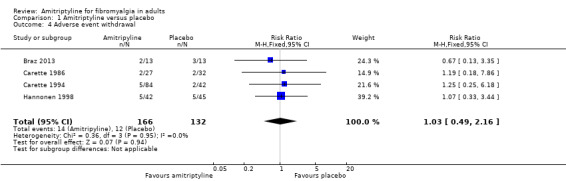
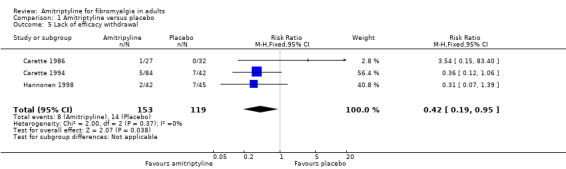
Main results: We included seven studies from the earlier review and two new studies (nine studies, 649 participants) of 6 to 24 weeks' duration, enrolling between 22 and 208 participants; none had 50 or more participants in each treatment arm. Two studies used a cross-over design. The daily dose of amitriptyline was 25 mg to 50 mg, and some studies had an initial titration period. There was no first or second tier evidence for amitriptyline in the treatment of fibromyalgia. Using third tier evidence the risk ratio (RR) for at least 50% pain relief, or equivalent, with amitriptyline compared with placebo was 3.0 (95% confidence interval (CI) 1.7 to 4.9), with an NNT) of 4.1 (2.9 to 6.7) (very low quality evidence). There were no consistent differences between amitriptyline and placebo or other active comparators for relief of symptoms such as fatigue, poor sleep, quality of life, or tender points. More participants experienced at least one adverse event with amitriptyline (78%) than with placebo (47%). The RR was 1.5 (1.3 to 1.8) and the NNH was 3.3 (2.5 to 4.9). Adverse event and all-cause withdrawals were not different, but lack of efficacy withdrawals were more common with placebo (12% versus 5%; RR 0.42 (0.19 to 0.95)) (very low quality evidence).
Authors' conclusions: Amitriptyline has been a first-line treatment for fibromyalgia for many years. The fact that there is no supportive unbiased evidence for a beneficial effect is disappointing, but has to be balanced against years of successful treatment in many patients with fibromyalgia. There is no good evidence of a lack of effect; rather our concern should be of overestimation of treatment effect. Amitriptyline will be one option in the treatment of fibromyalgia, while recognising that only a minority of patients will achieve satisfactory pain relief. It is unlikely that any large randomised trials of amitriptyline will be conducted in fibromyalgia to establish efficacy statistically, or measure the size of the effect.
INTRODUÇÃO: Essa é uma revisão atualizada da revisão da Cochrane originalmente publicada na Edição 12, 2012. Essa revisão considerou tanto fibromialgia e dor neuropática, mas a eficácia da amitriptilina para a dor neuropática é agora tratada em uma revisão separada. Amitriptilina é um antidepressivo tricíclico que é amplamente usado para tratar a fibromialgia, e é recomendado em muitos guidelines. É normalmente usado em doses inferiores àquelas que as drogas agem como antidepressivos. OBJETIVOS: Avaliar a eficácia analgésica da amitriptilina para o alívio da fibromialgia, e os eventos adversos associados com seu uso em ensaios clínicos. MÉTODOS DE BUSCA: Buscamos no CENTRAL, MEDLINE, e EMBASE em Março de 2015, juntamente com listas de referência de papéis recuperados, revisões sistemáticas anteriores e outras revisões, e registros de dois ensaios clínicos. Nós também usamos a nossa própria base procurando no banco de dados por estudos mais antigos. CRITÉRIO DE SELEÇÃO: Nós incluímos estudos randomizados, duplo‐cegos de duração mínima de quatro semanas comparando amitriptilina com placebo ou outro tratamento ativo na fibromialgia. COLETA DOS DADOS E ANÁLISES: Extraímos dados de eficácia e eventos adversos, e dois autores do estudo examinaram questões de qualidade do estudo de forma independente. Foram realizadas análises utilizando três níveis de evidência. Primeiro nível de evidência derivado de dados de reuniões com melhores padrões atuais e sujeitos a um risco mínimo de viés (resultado equivalente à redução da intensidade da dor substancial, análise de intenção de tratar, sem imputação para desistências; pelo menos 200 participantes na comparação, de 8 a 12 semanas de duração, projeto paralelo), o segundo nível de evidência com dados que não conseguiram cumprir um ou mais destes critérios e foram considerados em algum risco de viés, mas com números adequados na comparação, e terceiro nível a partir de dados envolvendo um pequeno número de participantes que foram considerados muito provável de ser tendencioso ou resultados de utilidade clínica limitados, ou ambos. Para eficácia, foi calculado o número necessário para tratar de benefício (NNT) e para o malefício foi calculado o número necessário para tratar de dano (NNH) para eventos adversos e desistências. Nós usamos um modelo de efeito fixo para a meta‐análise. PRINCIPAIS RESULTADOS: Nós incluímos sete estudos da revisão anterior e dois novos estudos (nove estudos, 649 participantes) com a duração de 6 a 24 semanas, registrando‐se entre 22 e 208 participantes; nenhum tinha 50 ou mais participantes em cada grupo de tratamento. Dois estudos usaram um modelo cross‐over. A dose diária de amitriptilina foi de 25 mg a 50 mg, e alguns estudos tem um período de titulação inicial. Não houve evidência de primeiro ou segundo nível da amitriptilina no tratamento da fibromialgia. Usando terceiro nível de evidência a razão de risco (RR) para alívio da dor de pelo menos 50%, ou equivalente, com amitriptilina em comparação com o placebo foi de 3,0 (intervalo de confiança de 95% (IC) 1,7 a 4,9), com um NNT de 4,1 (2,9 a 6.7) (evidência muito baixa qualidade). Não houve diferenças consistentes entre amitriptilina e placebo ou outros comparadores ativos para o alívio de sintomas como fadiga, falta de sono, qualidade de vida, ou tender points. Mais participantes experimentaram pelo menos um evento adverso com amitriptilina (78%) do que com placebo (47%). O RR era de 1,5 (1,3 a 1,8) e a NNH foi de 3,3 (2,5 a 4,9). Eventos adversos e todas as causas de abandono não foram diferentes, mas a falta de levantamentos de eficácia foram mais comuns com placebo (12% versus 5%; RR 0,42 (0,19 a 0,95)) (evidência de muito baixa qualidade). CONCLUSÃO DOS AUTORES: Amitriptilina tem sido um tratamento de primeira linha para a fibromialgia por muitos anos. O fato de que não há nenhuma evidência imparcial de suporte para um efeito benéfico é decepcionante, mas tem de ser equilibrado contra anos de tratamento com sucesso em muitos pacientes com fibromialgia. Não há boa evidência de uma falta de efeito; sim a nossa preocupação deve ser de superestimação do efeito do tratamento. Amitriptilina será uma opção no tratamento da fibromialgia, embora reconhecendo que apenas uma minoria dos pacientes vai conseguir alívio da dor. É pouco provável que quaisquer grandes ensaios clínicos de amitriptilina serão conduzidos na fibromialgia para estabelecer a eficácia estatistica ou medir o tamanho do efeito.
Contexte: Ceci est une version mise à jour de la revue Cochrane initialement publiée dans le numéro 12 de 2012. La revue originale portait à la fois sur la fibromyalgie et la douleur neuropathique, mais l'efficacité de l'amitriptyline pour traiter la douleur neuropathique est maintenant traité par une autre revue. L'amitriptyline est un antidépresseur tricyclique qui est largement utilisé pour traiter la fibromyalgie, et qui est préconisé dans de nombreuses recommandations. Il est généralement utilisé à des doses inférieures à celles auxquelles les médicaments agissent comme antidépresseurs.
Objectifs: Évaluation de l'efficacité analgésique de l'amitriptyline pour le soulagement de la fibromyalgie, et des effets indésirables associés à son utilisation dans les essais cliniques. STRATÉGIE DE RECHERCHE DOCUMENTAIRE: Nous avons fait des recherches dans CENTRAL, MEDLINE et Embase jusqu'en mars 2015, ainsi que dans les bibliographies des articles trouvés, des revues systématiques et autres revues antérieures, et dans deux registres d'essais cliniques. Nous avons également utilisé notre propre base de données de recherche manuelle pour trouver des études plus anciennes. CRITÈRES DE SÉLECTION: Nous avons inclus les études randomisées à double insu d'une durée d'au moins quatre semaines comparant l'amitriptyline à un placebo ou à un autre traitement actif contre la fibromyalgie. RECUEIL ET ANALYSE DES DONNÉES: Nous avons extrait les données relatives à l’efficacité et aux effets indésirables, et deux auteurs ont examiné les questions de qualité d'étude de manière indépendante. Nous avons procédé à une analyse en utilisant trois niveaux de preuves. Les preuves de premier niveau proviennent de données répondant aux meilleures normes de qualité actuelles et présentent un risque minimal de biais (le critère de jugement équivaut à une réduction substantielle de l'intensité de la douleur, l’analyse en intention de traiter sans imputation des abandons ; un nombre d’au moins 200 participants pour la comparaison, une durée de 8 à 12 semaines, une conception parallèle). Les preuves de deuxième niveau proviennent de données qui ne répondent pas à un ou plusieurs de ces critères et qui présentent un certain risque de biais, mais dont le nombre est suffisant dans la comparaison. Les preuves de troisième niveau impliquent des données portant sur un petit nombre de participants qui sont très susceptibles d'être biaisées ou qui utilisent des critères de jugement d’utilité clinique limitée, ou les deux. Pour l'efficacité, nous avons calculé le nombre de sujets à traiter pour obtenir un effet bénéfique (NST), et pour les effets néfastes, nous avons calculé le nombre nécessaire pour nuire (NNN) pour les effets indésirables et les abandons d’étude. Un modèle à effets fixes a été utilisé pour la méta‐analyse. RÉSULTATS PRINCIPAUX: Nous avons inclus sept études de la revue précédente et deux nouvelles études (neuf études, 649 participants) d'une durée de 6 à 24 semaines, comptant entre 22 et 208 participants ; aucune ne comptait 50 participants ou plus dans chaque groupe de traitement. Deux études ont utilisé une conception croisée. La dose quotidienne d'amitriptyline était de 25 à 50 mg, et certaines études comportaient une période initiale d'ajustement posologique. Il n'y avait pas de données probantes de premier ou de deuxième niveau pour l'amitriptyline dans le traitement de la fibromyalgie. Selon les données de troisième niveau, le risque relatif (RR) pour un soulagement de la douleur d'au moins 50 % ou équivalent, avec l'amitriptyline par rapport au placebo était de 3,0 (intervalle de confiance (IC) à 95 % de 1,7 à 4,9), avec un NST de 4,1 (2,9 à 6,7) (données probantes de très faible qualité). Il n'y avait pas de différences cohérentes entre l'amitriptyline et le placebo ou d'autres comparateurs actifs pour le soulagement de symptômes tels que la fatigue, le sommeil de mauvaise qualité, la qualité de vie ou la présence de points sensibles. Plus de participants ont subi au moins un effet indésirable avec l'amitriptyline (78 %) qu'avec le placebo (47 %). Le risque relatif était de 1,5 (1,3 à 1,8) et le nombre nécessaire pour nuire était de 3,3 (2,5 à 4,9). Les retraits pour cause d’effets indésirable et les retraits toutes causes confondues étaient similaires, mais les retraits pour manque d'efficacité étaient plus fréquents avec le placebo (12 % contre 5 % ; RR 0,42 (0,19 à 0,95)) (données probantes de très faible qualité).
Conclusions des auteurs: L'amitriptyline est un traitement de première intention de la fibromyalgie depuis de nombreuses années. Le fait qu'il n'y ait pas de preuve impartiale d'un effet bénéfique est décevant, mais doit être contrebalancé par les années de traitement réussi chez de nombreux patients atteints de fibromyalgie. Il n'existe pas de preuves satisfaisantes d'une absence d'effet ; nous devrions nous inquiéter davantage d'une surestimation de l'effet du traitement. L'amitriptyline sera une option dans le traitement de la fibromyalgie, tout en reconnaissant que seule une minorité des patients obtiendra un soulagement satisfaisant de la douleur. Il est peu probable que des essais randomisés de grande envergure soient menés pour mesurer statistiquement l’efficacité et l’ampleur de l’effet de l'amitriptyline pour le traitement de la fibromyalgie.
Antecedentes: Ésta es una versión actualizada de la revisión Cochrane original publicada en el número 12, 2012. Dicha revisión consideró la fibromialgia y el dolor neuropático, pero la eficacia de la amitriptilina para el dolor neuropático se trata actualmente en una revisión separada. La amitriptilina es un antidepresivo tricíclico que se utiliza ampliamente para tratar la fibromialgia y se recomienda en muchas guías. Por lo general, se utiliza en dosis inferiores a las dosis del fármaco como antidepresivo.
Objetivos: Evaluar la eficacia analgésica de la amitriptilina para aliviar la fibromialgia y los eventos adversos asociados con su uso en ensayos clínicos. MÉTODOS DE BÚSQUEDA: Se realizaron búsquedas en CENTRAL, MEDLINE y EMBASE hasta marzo de 2015, así como en las listas de referencias de los artículos recuperados, las revisiones sistemáticas anteriores y en otras revisiones, y en dos registros de ensayos clínicos. También se realizaron búsquedas manuales de los estudios más antiguos en las base de datos de los autores. CRITERIOS DE SELECCIÓN: Se incluyeron estudios aleatorios doble ciego de al menos cuatro semanas de duración, que compararon amitriptilina con placebo u otro tratamiento activo para la fibromialgia. OBTENCIÓN Y ANÁLISIS DE LOS DATOS: Se extrajeron los datos de eficacia y de los eventos adversos, y dos revisores examinaron de forma independiente aspectos de la calidad del estudio. Se realizó el análisis con tres niveles de pruebas. El primer nivel de evidencia se obtuvo a partir de los datos que cumplieron con los mejores estándares actuales y que tuvieron un riesgo de sesgo mínimo (un resultado equivalente a una reducción significativa en la intensidad del dolor, un análisis de intención de tratar sin imputación de los abandonos, al menos 200 participantes en la comparación, duración de ocho a 12 semanas, diseño paralelo); el segundo nivel a partir de los datos que no cumplieron con uno o más de estos criterios y que se consideró que tuvieron cierto riesgo de sesgo, pero con números adecuados en la comparación; y el tercer nivel a partir de los datos que incluyeron números pequeños de participantes y que se consideró que era muy probable que estuvieran sesgados o que utilizaran resultados de escasa utilidad clínica, o ambos. Para la eficacia, se calculó el número necesario a tratar para lograr un beneficio (NNTB), y para el daño se calculó el número necesario a tratar para causar daño (NNTD) para los eventos adversos y los abandonos. Para el metanálisis se utilizó un modelo de efectos fijos.
Resultados principales: Se incluyeron siete estudios de la revisión anterior y dos estudios nuevos (nueve estudios, 649 participantes) de seis a 24 semanas de duración, que incorporaron entre 22 y 208 participantes. Ninguno tuvo 50 o más participantes en cada brazo de tratamiento. Dos estudios utilizaron un diseño cruzado (cross‐over). La dosis diaria de amitriptilina fue de 25 mg a 50 mg, y algunos estudios tuvieron un período inicial de disminución gradual de la dosis. No hubo evidencia de primer o segundo nivel para la amitriptilina en el tratamiento de la fibromialgia. Al utilizar evidencia de tercer nivel, el cociente de riesgos (CR) para al menos el 50% de alivio del dolor, o un equivalente, con amitriptilina en comparación con placebo fue 3,0 (intervalo de confianza [IC] del 95%: 1,7 a 4,9), con un NNTB de 4,1 (2,9 a 6,7) (evidencia de calidad muy baja). No hubo diferencias consistentes entre la amitriptilina y placebo u otros comparadores activos para el alivio de los síntomas como fatiga, sueño deficiente, calidad de vida o puntos hipersensibles. Más participantes presentaron al menos un evento adverso con amitriptilina (78%) en comparación con placebo (47%). El CR fue 1,5 (1,3 a 1,8) y el NNTD fue 3,3 (2,5 a 4,9). Los abandonos por eventos adversos y por todas las causas no fueron diferentes, pero los abandonos por falta de eficacia fueron más frecuentes con placebo (12% versus 5%; CR 0,42 [0,19 a 0,95]) (evidencia de calidad muy baja).
Conclusiones de los autores: La amitriptilina ha sido un tratamiento de primera línea para la fibromialgia durante muchos años. El hecho de que no exista evidencia no sesgada para apoyar un efecto beneficioso es decepcionante, aunque se debe considerar en relación con los años de tratamiento exitoso en muchos pacientes con fibromialgia. No existe evidencia convincente de una falta de efecto; más bien la preocupación debe ser la sobrestimación del efecto del tratamiento. La amitriptilina será una opción en el tratamiento de la fibromialgia, aunque se reconoce que solo una minoría de los pacientes logrará un alivio satisfactorio del dolor. Es poco probable que se realicen ensayos aleatorios grandes de la amitriptilina en la fibromialgia para establecer su eficacia desde el punto de vista estadístico, o para medir el tamaño del efecto.
Copyright © 2019 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
SD has no conflicts relating to this review or any similar product.
PW has no conflicts relating to this review or any similar product.
RAM has no conflicts relating to this review or any similar product.
DA has no conflicts relating to this review or any similar product.
PC has received research support from industry sources at various times but none related to this review.
For transparency SD, PW and RAM have received research support from charities, government, and industry sources at various times, but none relate to this review. We are funded by the NIHR for work on a series of reviews informing the unmet need of chronic pain and providing the evidence for treatments of pain.
Figures
References
References to studies included in this review
Braz 2013 {published data only}
Carette 1986 {published data only}
-
- Carette S, McCain GA, Bell DA, Fam AG. Evaluation of amitriptyline in primary fibrositis. A double‐blind, placebo‐controlled study. Arthritis and Rheumatism 1986;29(5):655‐9. - PubMed
Carette 1994 {published data only}
-
- Carette S, Bell MJ, Reynolds WJ, Haraoui B, McCain GA, Bykerk VP, et al. Comparison of amitriptyline, cyclobenzaprine, and placebo in the treatment of fibromyalgia. A randomized, double‐blind clinical trial. Arthritis and Rheumatism 1994;37(1):32‐40. - PubMed
Carette 1995 {published data only}
-
- Carette S, Oakson G, Guimont C, Steriade M. Sleep electroencephalography and the clinical response to amitriptyline in patients with fibromyalgia. Arthritis and Rheumatism 1995;38(9):1211‐7. - PubMed
de Zanette 2014 {published data only}
-
- Cauma W (Principle investigator). Immune‐Pineal Axis Function in Fibromyalgia. www.clinicaltrials.gov/ct2/show/NCT02041455?term=NCT02041455&rank=1 (accessed 30 Mar 15) 2014. [CTG: NCT02041455]
-
- Zanette SA, Vercelino R, Laste G, Rozisky JR, Schwertner A, Machado CB, et al. Melatonin analgesia is associated with improvement of the descending endogenous pain‐modulating system in fibromyalgia: a phase II, randomized, double‐dummy, controlled trial. BMC Pharmacology and Toxicology 2014;15:40. [DOI: 10.1186/2050-6511-15-40] - DOI - PMC - PubMed
Ginsberg 1996 {published data only}
-
- Ginsberg F, Mancaux A, Joos E, Vanhove P, Famey J‐P. A randomized placebo‐controlled trial of sustained‐release amitriptyline in fibromyalgia. Journal of Musculoskeletal Pain 1996;4(3):37‐47.
Goldenberg 1986 {published data only}
-
- Goldenberg DL, Felson DT, Dinerman H. A randomized, controlled trial of amitriptyline and naproxen in the treatment of patients with fibromyalgia. Arthritis and Rheumatism 1986;29(11):1371‐7. - PubMed
Goldenberg 1996 {published data only}
-
- Goldenberg D, Mayskiy M, Mossey C, Ruthazer R, Schmid C. A randomized, double‐blind crossover trial of fluoxetine and amitriptyline in the treatment of fibromyalgia. Arthritis and Rheumatism 1996;39(11):1852‐9. - PubMed
Hannonen 1998 {published data only}
-
- Hannonen P, Malminiemi K, Yli‐Kerttula U, Isomeri R, Roponen P. A randomized, double‐blind, placebo‐controlled study of moclobemide and amitriptyline in the treatment of fibromyalgia in females without psychiatric disorder. British Journal of Rheumatology 1998;37(12):1279‐86. - PubMed
References to studies excluded from this review
Fors 2002 {published data only}
-
- Fors EA, Sexton H, Götestam KG. The effect of guided imagery and amitriptyline on daily fibromyalgia pain: a prospective, randomized, controlled trial. Journal of Psychiatric Research 2002;36(3):179‐87. - PubMed
Hampf 1989 {published data only}
Heymann 2001 {published data only}
-
- Heymann RE, Helfenstein M, Feldman D. A double‐blind, randomized, controlled study of amitriptyline, nortriptyline and placebo in patients with fibromyalgia. An analysis of outcome measures. Clinical and Experimental Rheumatology 2001;19(6):697‐702. - PubMed
Isomeri 1993 {published data only}
-
- Isomeri R, Mikkelsson M, Latikka P, Kammonen K. Effects of amitriptyline and cardiovascular fitness training on pain in patients with primary fibromyalgia. Journal of Musculoskeletal Pain 1993;1(3/4):253‐60.
Jaeschke 1991 {published data only}
-
- Jaeschke R, Adachi J, Guyatt G, Keller J, Wong B. Clinical usefulness of amitriptyline in fibromyalgia: the results of 23 N‐of‐1 randomized controlled trials. Journal of Rheumatology 1991;18(3):447‐51. - PubMed
Kempenaers 1994 {published data only}
-
- Kempenaers C, Simenon G, Vander Elst M, Fransolet L, Mingard P, Maertelaer V, et al. Effect of an antidiencephalon immune serum on pain and sleep in primary fibromyalgia. Neuropsychobiology 1994;30(2‐3):66‐72. - PubMed
McQuay 1992 {published data only}
-
- McQuay HJ, Carroll D, Glynn CJ. Low dose amitriptyline in the treatment of chronic pain. Anaesthesia 1992;47(8):646‐52. - PubMed
McQuay 1993 {published data only}
-
- McQuay HJ, Carroll D, Glynn CJ. Dose‐response for analgesic effect of amitriptyline in chronic pain. Anaesthesia 1993;48(3):281‐5. - PubMed
Özerbil 2006 {published data only}
-
- Özerbil O, Okudan N, Gökbel H, Levendoğlu F. Comparison of the effects of two antidepressants on exercise performance of the female patients with fibromyalgia. Clinical Rheumatology 2006;25(4):495‐7. - PubMed
Pilowsky 1982 {published data only}
-
- Pilowsky I, Hallett EC, Bassett DL, Thomas PG, Penhall RK. A controlled study of amitriptyline in the treatment of chronic pain. Pain 1982;14(2):169‐79. - PubMed
Pilowsky 1990 {published data only}
-
- Pilowsky I, Barrow CG. A controlled study of psychotherapy and amitriptyline used individually and in combination in the treatment of chronic intractable, 'psychogenic' pain. Pain 1990;40(1):3‐19. - PubMed
Scudds 1989 {published data only}
-
- Scudds RA, McCain GA, Rollman GB, Harth M. Improvements in pain responsiveness in patients with fibrositis after successful treatment with amitriptyline. Journal of Rheumatology Supplement 1989;19:98‐103. - PubMed
Zitman 1990 {published data only}
-
- Zitman FG, Linssen AC, Edelbroek PM, Stijnen T. Low dose amitriptyline in chronic pain: the gain is modest. Pain 1990;42(1):35‐42. - PubMed
Zitman 1991 {published data only}
-
- Zitman FG, Linssen AC, Edelbroek PM, Kempen GM. Does addition of low‐dose flupentixol enhance the analgetic effects of low‐dose amitriptyline in somatoform pain disorder?. Pain 1991;47(1):25‐30. - PubMed
Ҫapaci 2002 {published data only}
-
- Ҫapaci K, Hepgüler S. Comparison of the effects of amitriptyline and paroxetine in the treatment of fibromyalgia syndrome. The Pain Clinic 2002;14(3):223‐8.
References to studies awaiting assessment
Ataoğlu 1997 {published data only}
-
- Ataoglu S, Ataoglu A, Erdogan F, Sarac J. Comparison of paroxetine, amitriptyline in the treatment of fibromyalgia. Turkish Journal of Medical Science 1997;27(6):535‐9.
Jang 2010 {published data only}
-
- Jang ZY, Li CD, Qiu L, Guo JH, He LN, Yue Y, et al. Combination of acupuncture, cupping and medicine for treatment of fibromyalgia syndrome: a multi‐central randomized controlled trial. Zhongguo Zhen Jiu [Chinese Acupuncture and Moxibustion] 2010;30(4):265‐9. - PubMed
NCT00381199 {published data only}
-
- Ware MA (Principle Investigator). Nabilone versus amitriptyline in improving quality of sleep in patients with fibromyalgia. www.clinicaltrials.gov/ct2/show/NCT00381199?term=NCT00381199&rank=1 (accessed 30 March 2015) 2007. [CTG: NCT00381199]
Additional references
Dechartres 2013
Dworkin 2008
Hausser 2011
Higgins 2003
Higgins 2011
-
- Higgins JPT, Green S (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Altman DG, Sterne JAC editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Jadad 1996a
-
- Jadad AR, Carroll D, Moore RA, McQuay H. Developing a database of published reports of randomised clinical trials in pain research. Pain 1996;66(2‐3):239‐46. - PubMed
Jadad 1996b
-
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Controlled Clinical Trials 1996;17(1):1‐12. [DOI: ] - PubMed
Kalso 2013
Kim 2015
Kjaergard 2001
-
- Kjaergard LL, Villumsen J, Gluud C. Reported methodologic quality and discrepancies between large and small randomized trials in meta‐analyses. Annals of Internal Medicine 2001;135(11):982‐9. - PubMed
Koroschetz 2011
L'Abbé 1987
-
- L'Abbé KA, Detsky AS, O'Rourke K. Meta‐analysis in clinical research. Annals of Internal Medicine 1987;107:224‐33. - PubMed
Lunn 2014
McQuay 1998
-
- McQuay H, Moore R. An evidence‐based resource for pain relief. Oxford: Oxford University Press, 1998. [ISBN: 0‐19‐263048‐2]
Moore 1998
Moore 2008
-
- Moore RA, Barden J, Derry S, McQuay HJ. Managing potential publication bias. In: McQuay HJ, Kalso E, Moore RA editor(s). Systematic Reviews in Pain Research: Methodology Refined. Seattle: IASP Press, 2008:15‐24. [ISBN: 978–0–931092–69–5]
Moore 2009
Moore 2010a
-
- Moore RA, Eccleston C, Derry S, Wiffen P, Bell RF, Straube S, et al. ACTINPAIN Writing Group of the IASP Special Interest Group on Systematic Reviews in Pain Relief, Cochrane Pain, Palliative and Supportive Care Systematic Review Group Editors. "Evidence" in chronic pain ‐ establishing best practice in the reporting of systematic reviews. Pain 2010;150(3):386‐9. [DOI: 10.1016/j.pain.2010.05.011] - DOI - PubMed
Moore 2010b
-
- Moore RA, Moore OA, Derry S, Peloso PM, Gammaitoni AR, Wang H. Responder analysis for pain relief and numbers needed to treat in a meta‐analysis of etoricoxib osteoarthritis trials: bridging a gap between clinical trials and clinical practice. Annals of the Rheumatic Diseases 2010;69(2):374‐9. [DOI: 10.1136/ard.2009.107805] - DOI - PMC - PubMed
Moore 2010c
Moore 2010d
Moore 2011a
-
- Moore RA, Straube S, Paine J, Derry S, McQuay HJ. Minimum efficacy criteria for comparisons between treatments using individual patient meta‐analysis of acute pain trials: examples of etoricoxib, paracetamol, ibuprofen, and ibuprofen/paracetamol combinations after third molar extraction. Pain 2011;152(5):982‐9. [DOI: ] - PubMed
Moore 2011b
Moore 2012b
Moore 2013a
Moore 2013b
Moore 2014a
-
- Moore RA, Derry S, Taylor RS, Straube S, Phillips CJ. The costs and consequences of adequately managed chronic non‐cancer pain and chronic neuropathic pain. Pain Practice 2014;14(1):79‐94. - PubMed
Moore 2014b
Moore 2014c
Moore 2015
Nishishinya 2008
Nuesch 2010
Nüesch 2010
Onghena 1992
-
- Onghena P, Houdenhove B. Antidepressant‐induced analgesia in chronic non‐malignant pain: a meta‐analysis of 39 placebo‐controlled studies. Pain 1992;49:205‐20. - PubMed
PaPaS 2012
-
- PaPaS author and referee guidance. http://papas.cochrane.org/papas‐documents (accessed 9 March 2015).
PCA 2014
-
- Anonymous. Prescription Cost Analysis, England 2013. Available at: hscic.gov.uk/catalogue/PUB13887/pres‐cost‐anal‐eng‐2013‐rep.pdf (Accessed 9 March 2015). Health and Social Care Information Centre, 2014:100‐1. [ISBN: 978‐1‐78386‐089‐0]
Queiroz 2013
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Schünemann 2011
-
- Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, Guyatt GH. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Straube 2010
Straube 2011
Sultan 2008
Vos 2012
-
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380(9859):2163‐96. [DOI: 10.1016/S0140-6736(12)61729-2] - DOI - PMC - PubMed
Wiffen 2013
Wolfe 1990
-
- Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis and Rheumatism 1990;33:160‐72. - PubMed
Wolfe 2010
Wolfe 2013
References to other published versions of this review
McQuay 1996
-
- McQuay HJ, Tramer M, Nye BA, Carroll D, Wiffen PJ, Moore RA. A systematic review of antidepressants in neuropathic pain. Pain 1996;68:217‐27. - PubMed
Moore 2012a
Publication types
LinkOut - more resources
Full Text Sources