

Right Heart Failure Following Left Ventricular Device Implantation: Natural History, Risk Factors, and Outcomes: An Analysis of the STS INTERMACS Database
- PMID: 35658464
- PMCID: PMC9233112
- DOI: 10.1161/CIRCHEARTFAILURE.121.008706
Right Heart Failure Following Left Ventricular Device Implantation: Natural History, Risk Factors, and Outcomes: An Analysis of the STS INTERMACS Database
Abstract
Background: Our current understanding of right heart failure (RHF) post-left ventricular assist device (LVAD) is lacking. Recently, a new Interagency Registry for Mechanically Assisted Circulatory Support definition of RHF was introduced. Based on this definition, we investigated natural history, risk factors, and outcomes of post-LVAD RHF.
Methods: Patients implanted with continuous flow LVAD between June 2, 2014, and June 30, 2016 and registered in the Interagency Registry for Mechanically Assisted Circulatory Support/Society of Thoracic Surgeons Database were included. RHF incidence and predictors, and survival after RHF were assessed. The manifestations of RHF which were separately analyzed were elevated central venous pressure, peripheral edema, ascites, and use of inotropes.
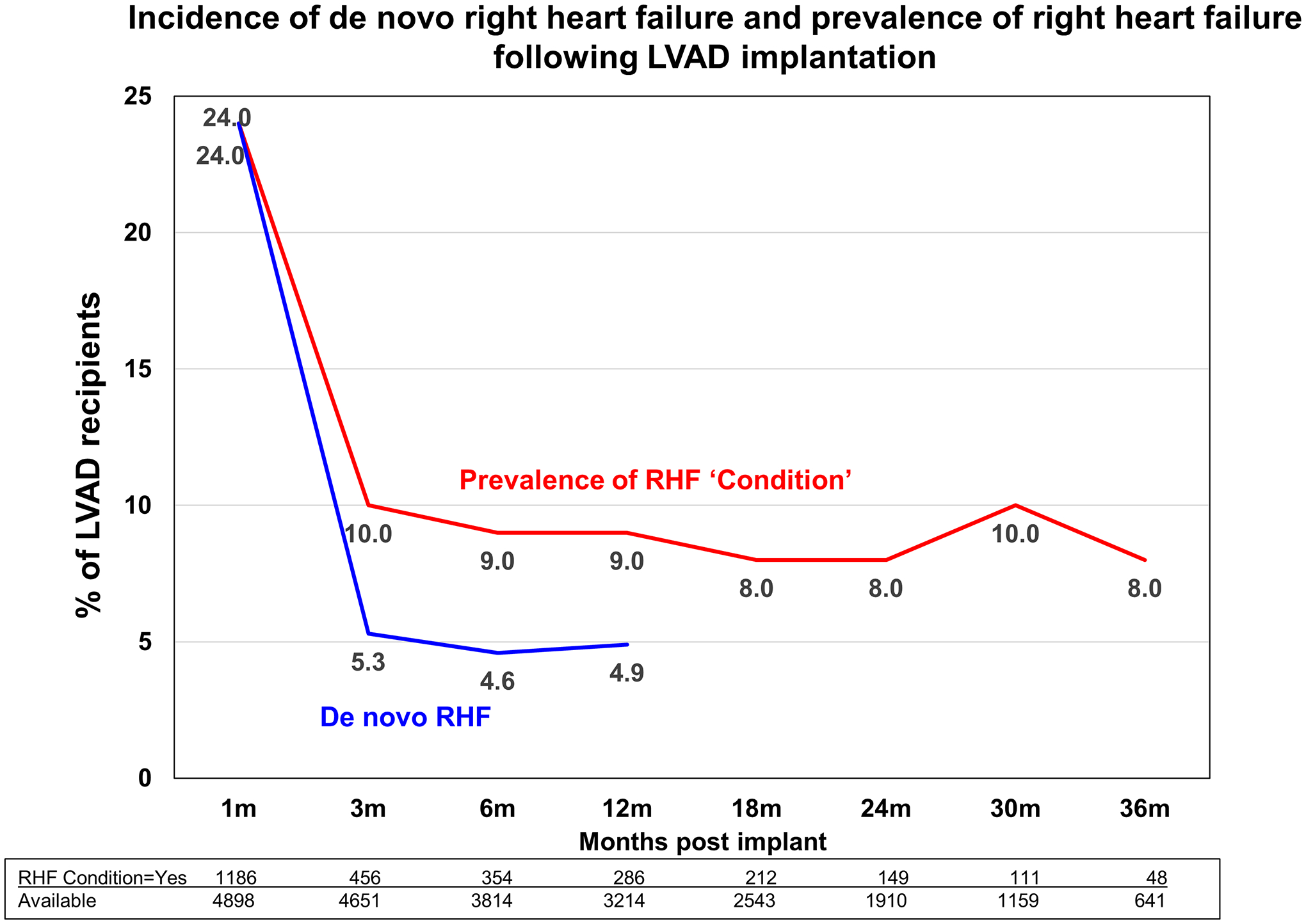
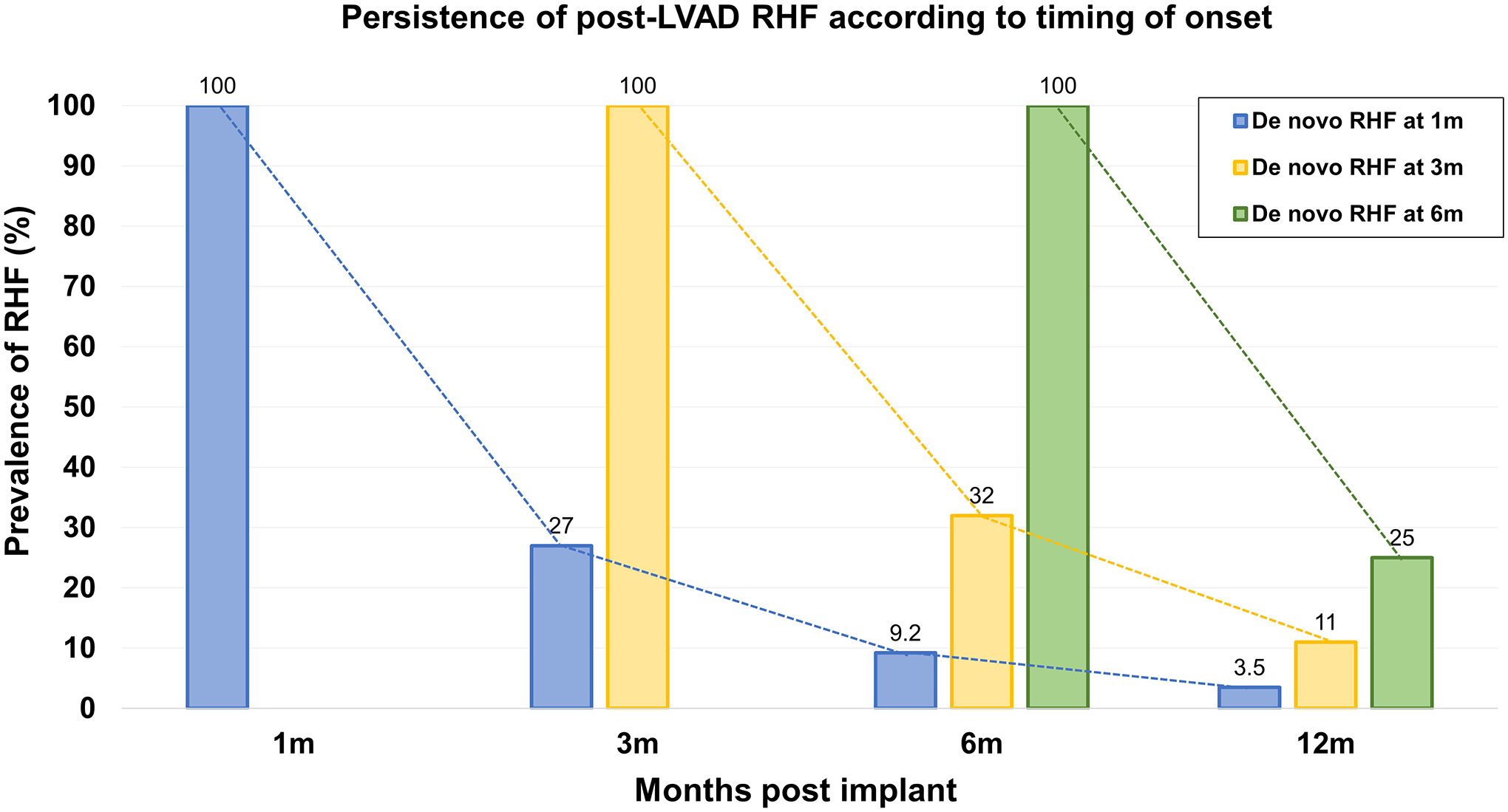
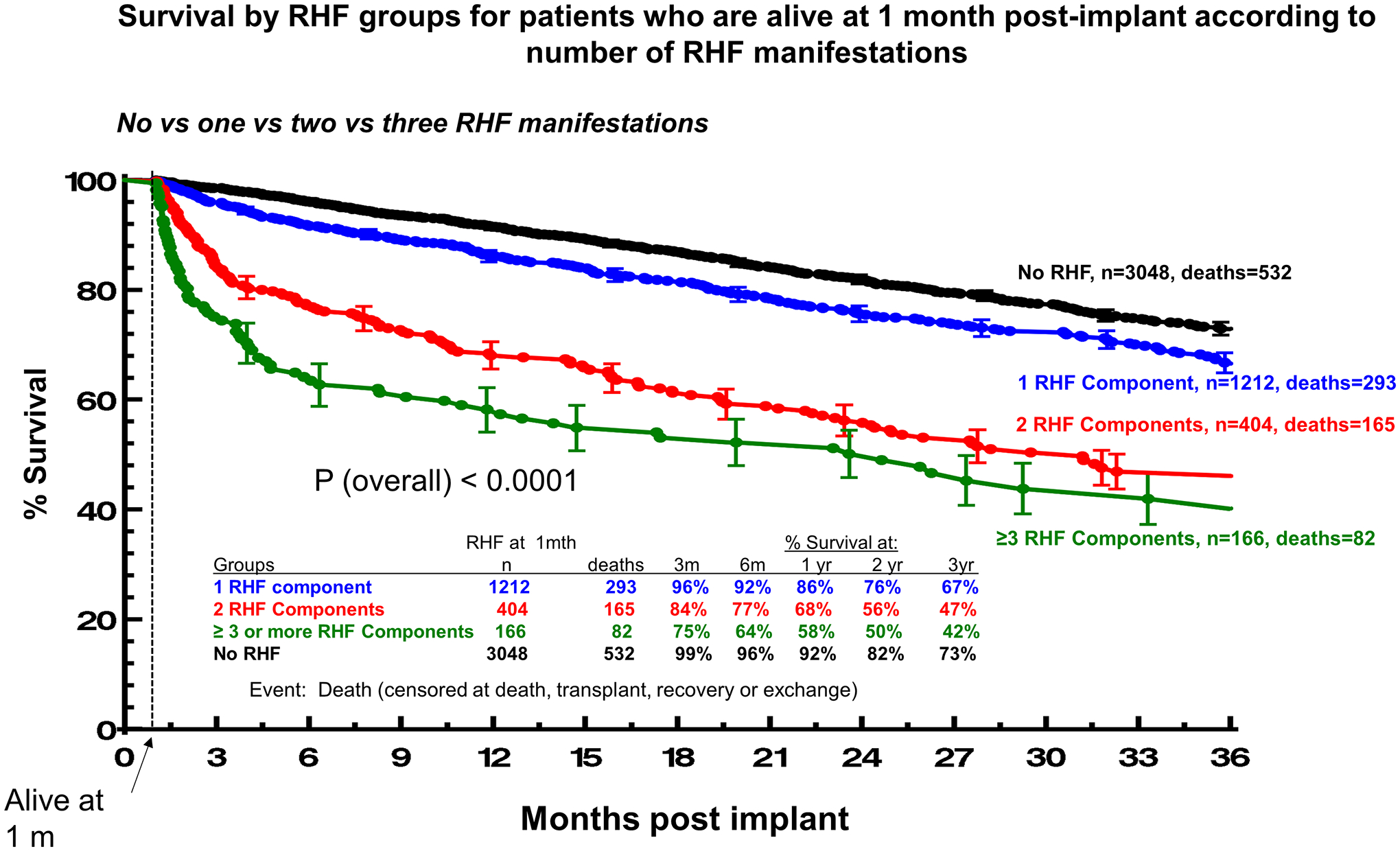
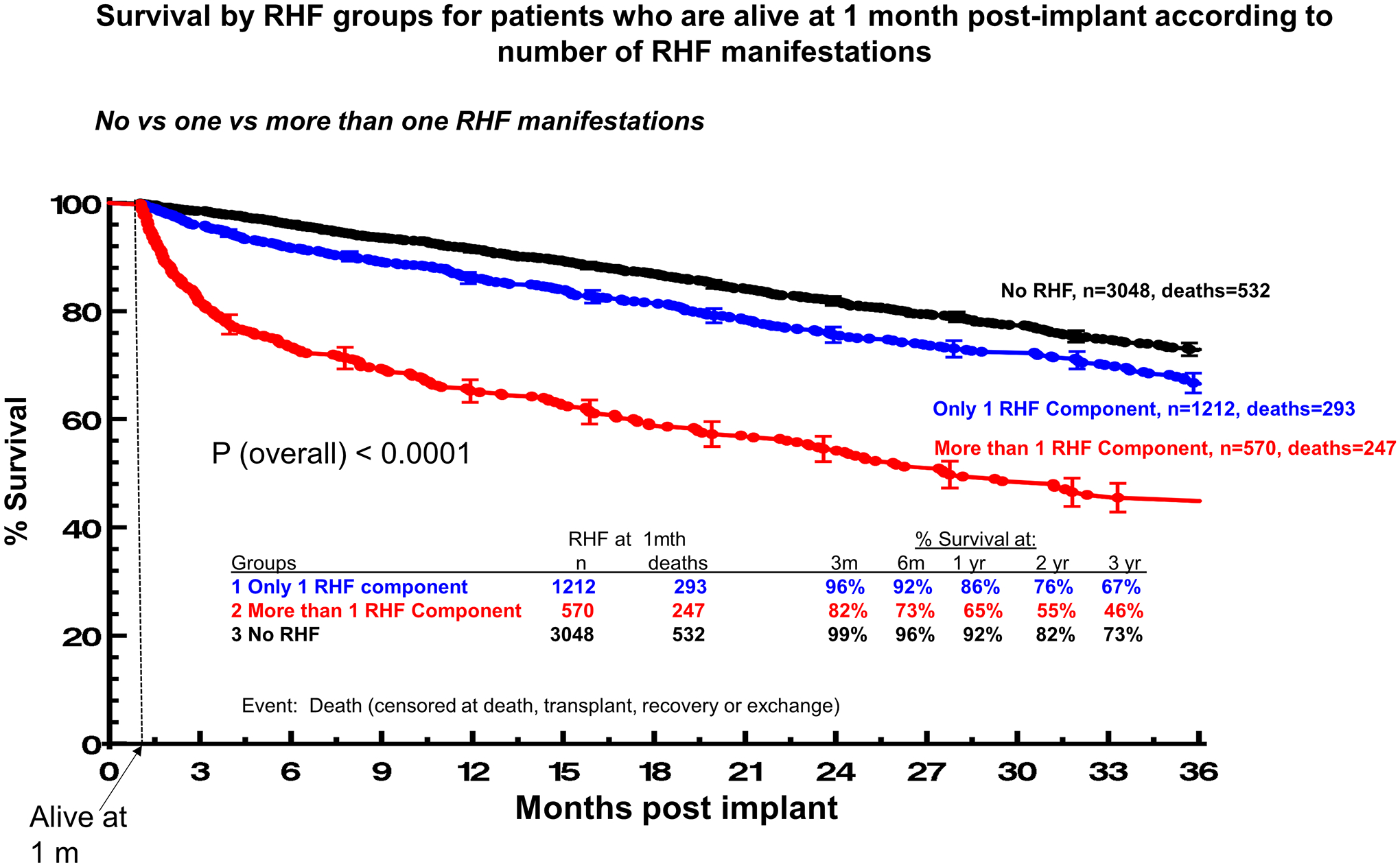
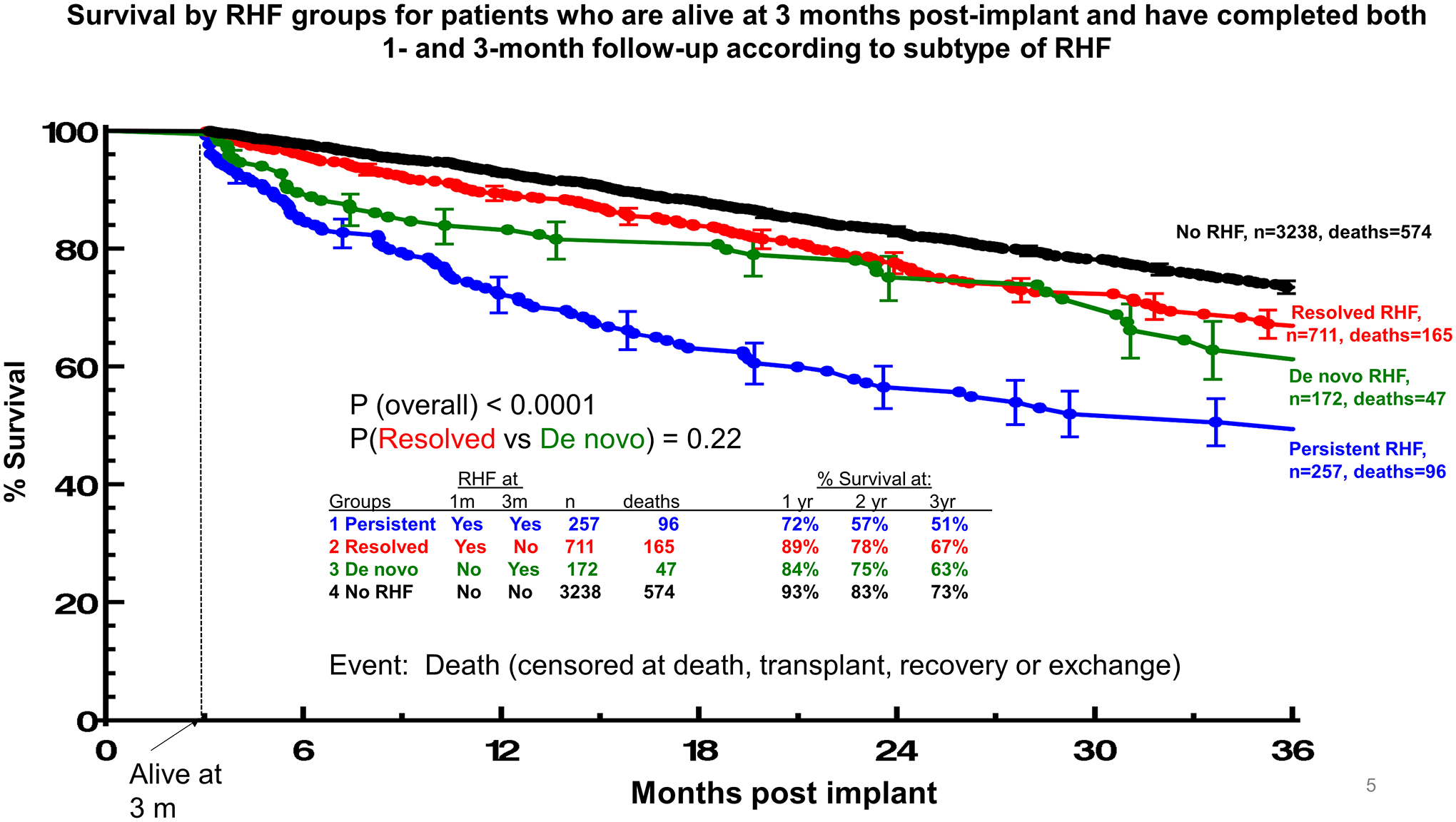
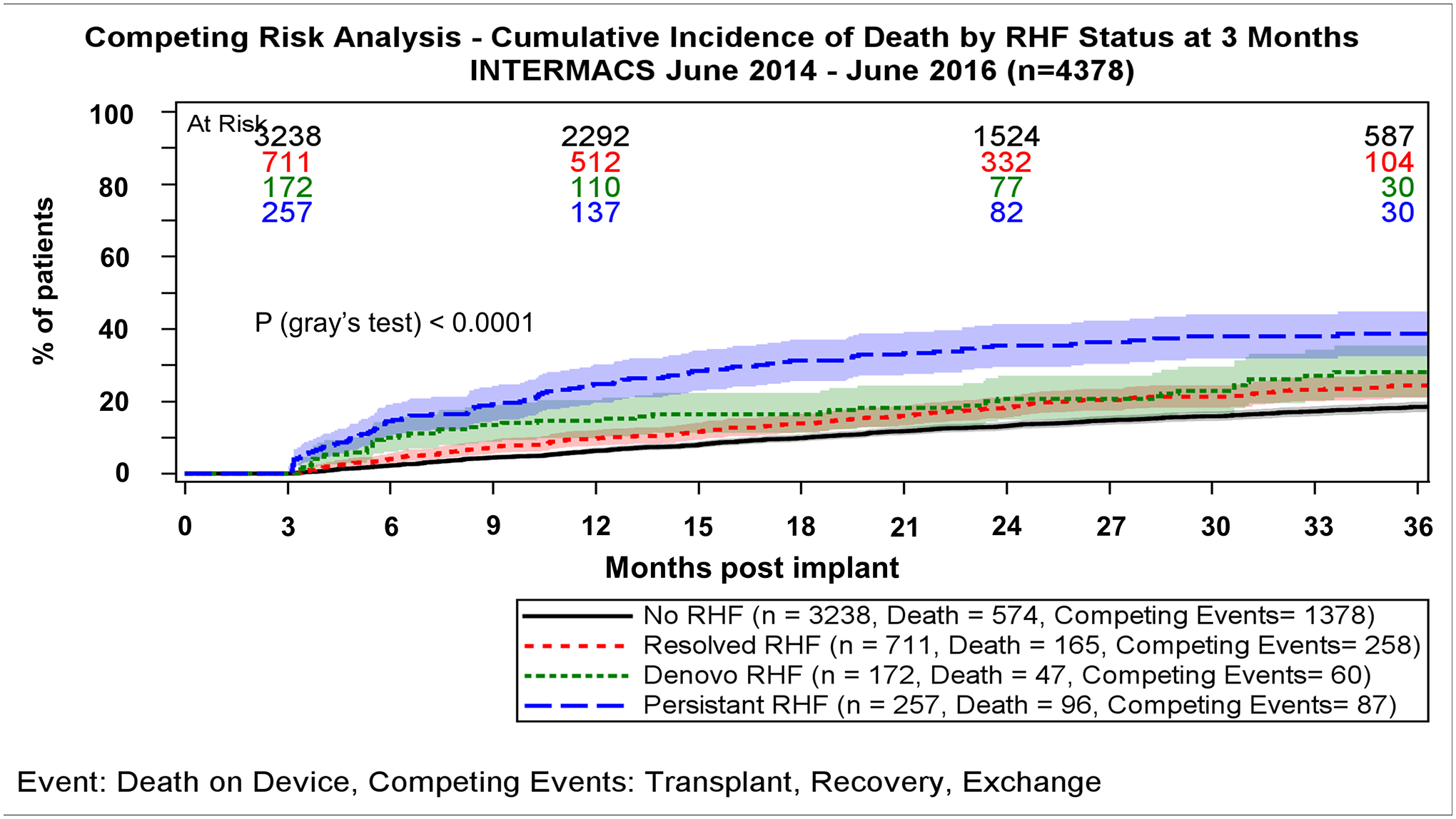
Results: Among 5537 LVAD recipients (mean 57±13 years, 49% destination therapy, support 18.9 months) prevalence of 1-month RHF was 24%. Of these, RHF persisted at 12 months in 5.3%. In contrast, de novo RHF, first identified at 3 months, occurred in 5.1% and persisted at 12 months in 17% of these, and at 6 months occurred in 4.8% and persisted at 12 months in 25%. Higher preimplant blood urea nitrogen (ORs,1.03-1.09 per 5 mg/dL increase; P<0.0001), previous tricuspid valve repair/replacement (ORs, 2.01-10.09; P<0.001), severely depressed right ventricular systolic function (ORs,1.17-2.20; P=0.004); and centrifugal versus axial LVAD (ORs,1.15-1.78; P=0.001) represented risk factors for RHC incidence at 3 months. Patients with persistent RHF at 3 months had the lowest 2-year survival (57%) while patients with de novo RHF or RHF which resolved by 3 months had more favorable survival outcomes (75% and 78% at 2 years, respectively; P<0.001).
Conclusions: RHF at 1 or 3 months post-LVAD was a common and frequently transient condition, which, if resolved, was associated with relatively favorable prognosis. Conversely, de novo, late RHF post-LVAD (>6 months) was more frequently a persistent disorder and associated with increased mortality. The 1-, 3-, and 6-month time points may be used for RHF assessment and risk stratification in LVAD recipients.
Keywords: edema; heart failure; hepatomegaly; prevalence; prognosis.
Figures
References
-
- Kormos RL, Teuteberg JJ, Pagani FD, Russell SD, John R, Miller LW, Massey T, Milano CA, Moazami N, Sundareswaran KS, et al. ; HeartMate II Clinical Investigators. Right ventricular failure in patients with the HeartMate II continuous-flow left ventricular assist device: incidence, risk factors, and effect on outcomes. J Thorac Cardiovasc Surg. 2010;139:1316–1324. - PubMed
-
- Teuteberg JJ, Studdard G, Kiernan M, Oliveria G, Rame E, Alturi P, Gaffey A, Grandin EW, Kirklin J, Myers S, et al. The Incidence of Early and Late Clinical Right Heart Failure and the Impact on Survival After Continuous Flow Mechanical Support: Insights from the New INTERMACS Definition of Right Heart Failure. J Heart Lung Transplant. 2017;36:356. Abstract
-
- Takeda K, Takayama H, Colombo PC, Jorde UP, Yuzefpolskaya M, Fukuhara S, Manicini DM, Naka Y. Late right heart failure during support with continuous-flow left ventricular assist devices adversely affects posttransplant outcome. J Heart Lung Transplant. 2015;34:667–674. - PubMed
-
- Kapelios CJ, Charitos C, Kaldara E, Malliaras K, Nana E, Pantsios C, Repasos E, Tsamatsoulis M, Toumanidis S, Nanas JN. Late-onset right ventricular dysfunction after mechanical support by a continuous-flow left ventricular assist device. J Heart Lung Transplant. 2015;34:1604–1610. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
