

Delivery outcomes associated with maternal congenital heart disease, 2000-2018
- PMID: 35658780
- PMCID: PMC9691578
- DOI: 10.1080/14767058.2022.2081803
Delivery outcomes associated with maternal congenital heart disease, 2000-2018
Abstract
Purpose: To characterize temporal trends and outcomes of delivery hospitalization with maternal congenital heart disease (CHD).
Materials and methods: For this repeated cross-sectional analysis, deliveries to women aged 15-54 years with maternal CHD were identified in the 2000-2018 National Inpatient Sample. Temporal trends in maternal CHD were analyzed using joinpoint regression to estimate the average annual percentage change (AAPC) with 95% CIs. The relationship between maternal CHD and several adverse maternal outcomes was analyzed with log-linear regression models. Risk for adverse outcomes in the setting of maternal CHD was further characterized based on additional diagnoses of cardiac comorbidity including congestive heart failure, arrhythmia, valvular disease, pulmonary disorders, and history of thromboembolism.
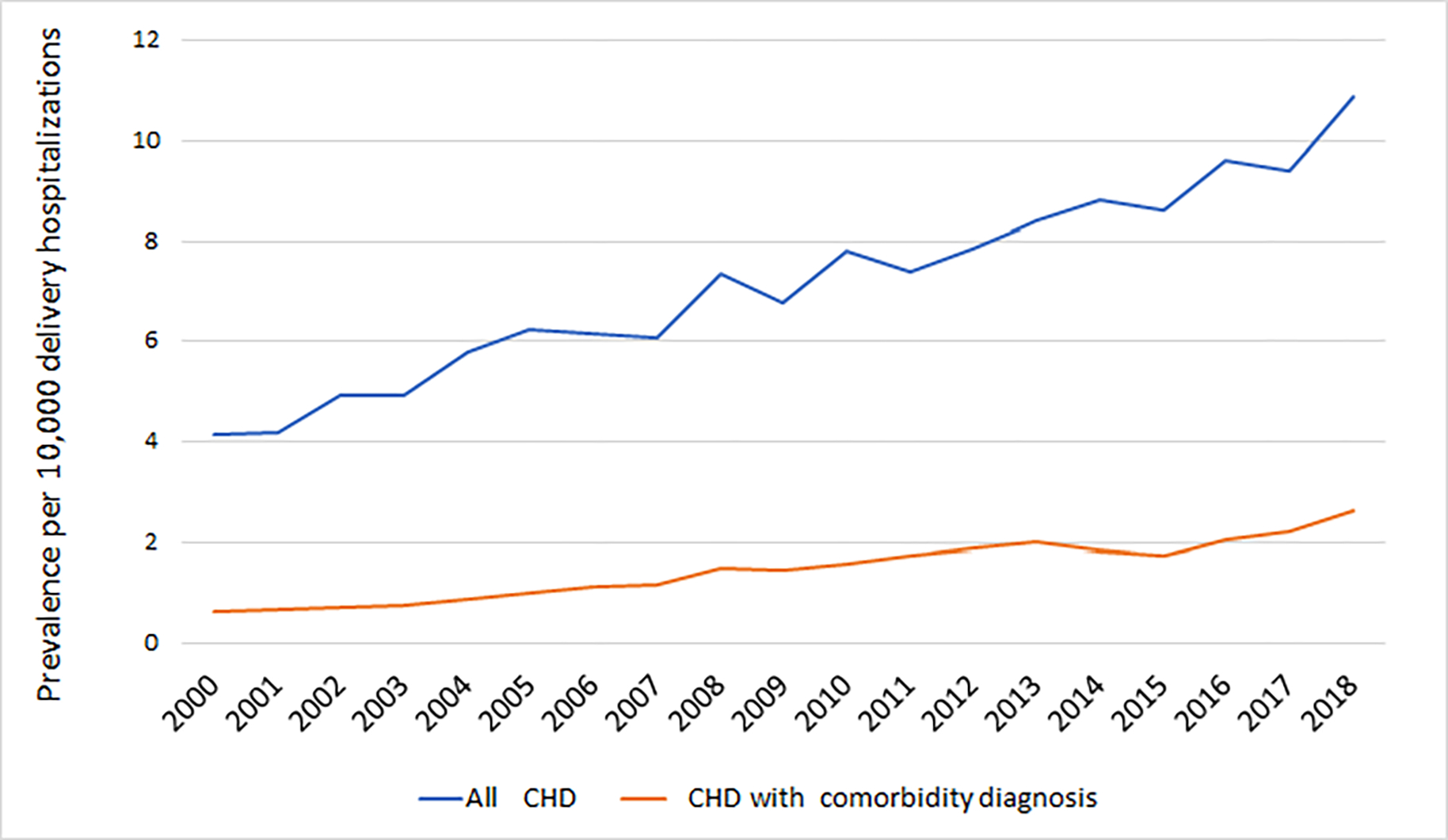
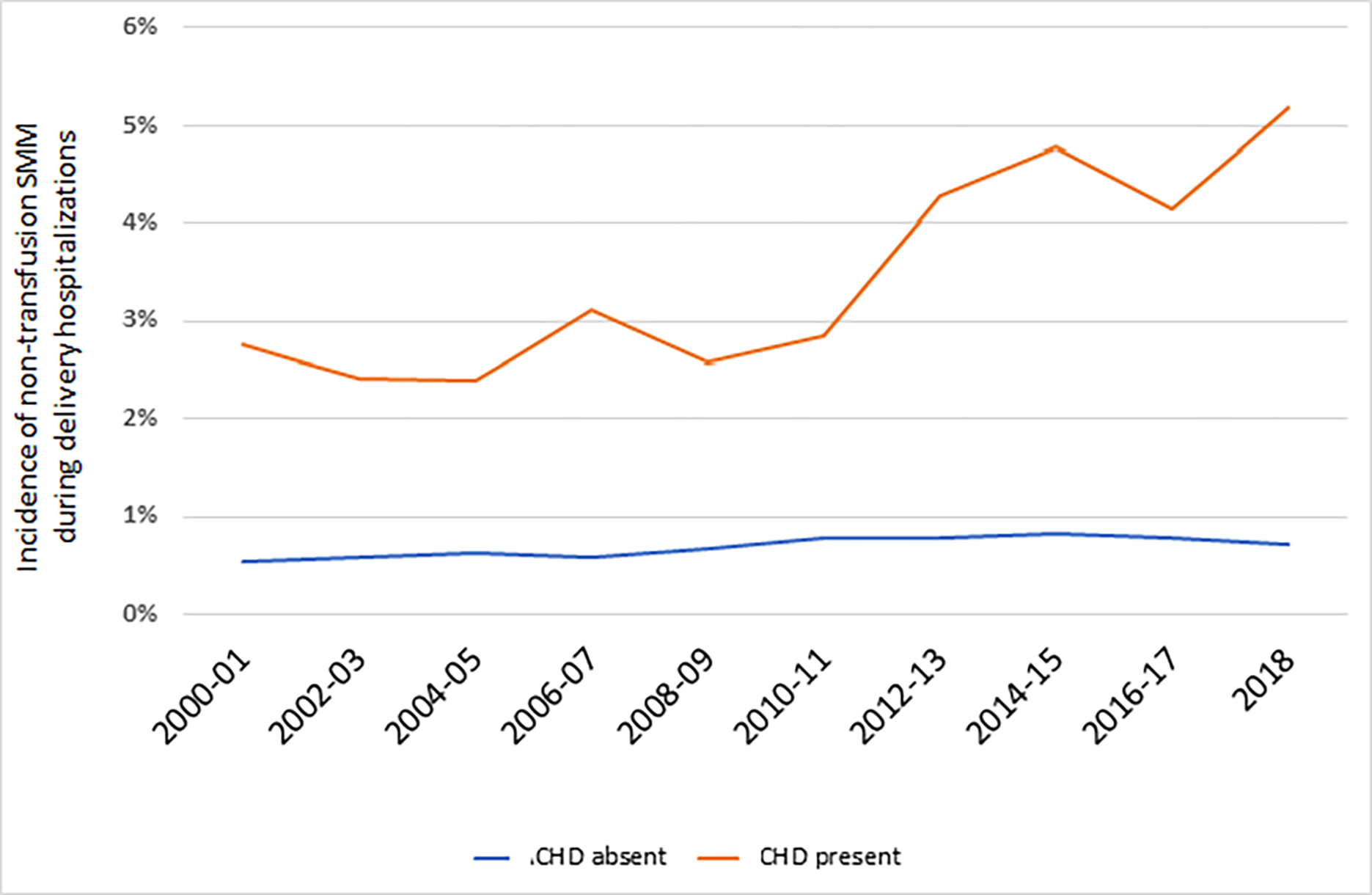
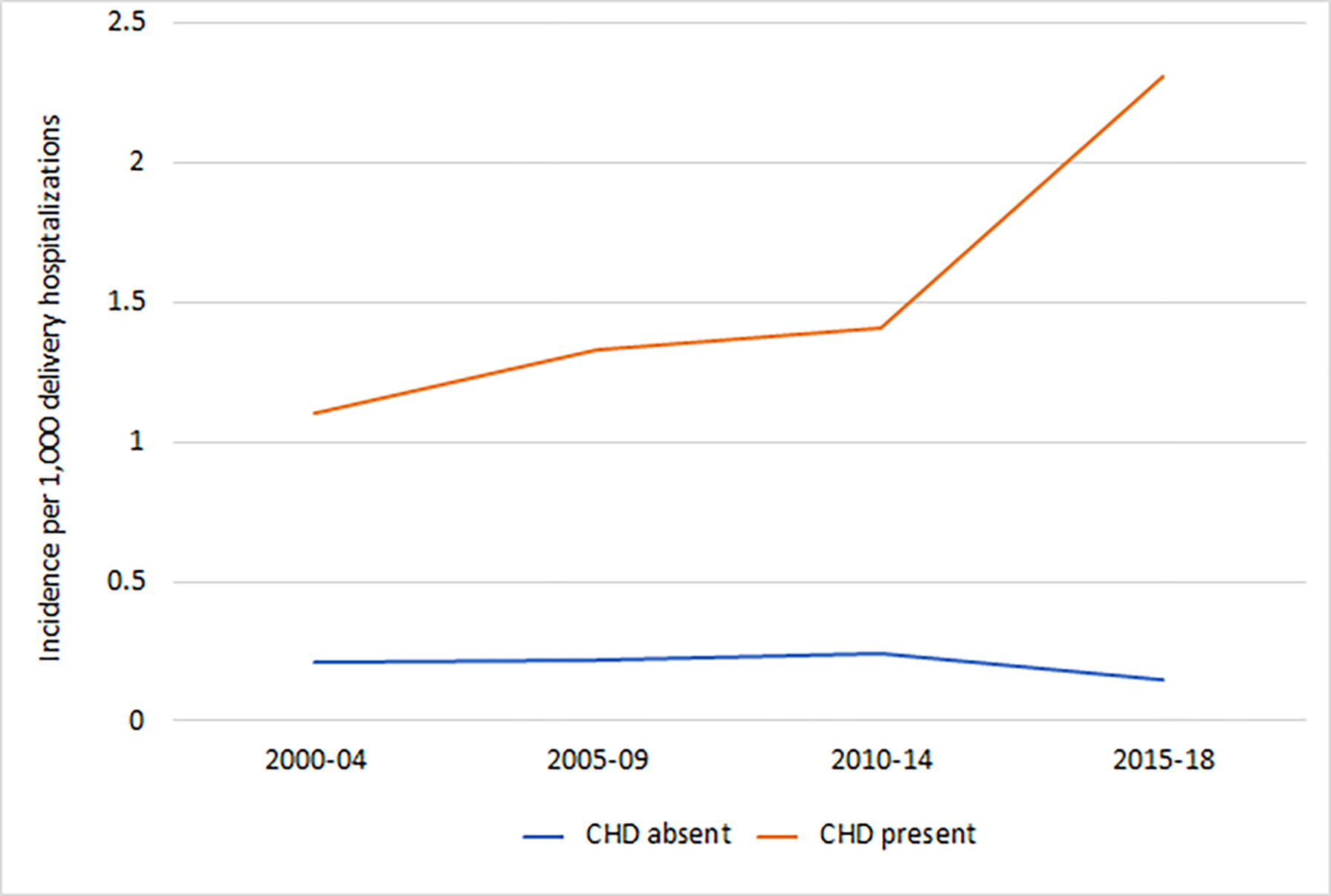
Results: Of 73,109,790 delivery hospitalizations, 51,841 had a diagnosis of maternal CHD (7.1 per 10,000). Maternal CHD rose from 4.2 to 10.9 per 10,000 deliveries (AAPC 4.8%, 95% CI 4.2%, 5.4%). Maternal CHD deliveries with a cardiac comorbidity diagnosis also increased from 0.6 to 2.6 per 10,000 from 2000 to 2018 (AAPC 8.4%, 95% CI 6.3%, 10.6%). Maternal CHD was associated with severe maternal morbidity (adjusted risk ratios [aRR] 4.97, 95% CI 4.75, 5.20), cardiac severe maternal morbidity (aRR 7.65, 95% CI 7.14, 8.19), placental abruption (aRR 1.30, 95% 1.21, 1.38), preterm delivery (aRR 1.47, 95% CI 1.43, 1.51), and transfusion (aRR 2.28, 95% CI 2.14, 2.42). Risk for severe morbidity (AAPC 4.7%, 95% CI 2.5%, 6.9%) and cardiac severe morbidity (AAPC 4.7%, 95% CI 2.5%, 6.9%) increased significantly among women with maternal CHD over the study period. The presence of cardiac comorbidity diagnoses was associated with further increased risk.
Conclusion: Maternal CHD is becoming more common among US deliveries. Among deliveries with maternal CHD, risk for severe morbidity is increasing. These findings support that an increasing burden of risk from maternal CHD in the obstetric population.
Keywords: Adult congenital heart disease; maternal morbidity; pregnancy.
Conflict of interest statement
Figures
References
-
- Benjamin EJ, Virani SS, Callaway CW, et al. Heart Disease and Stroke Statistics—2018 Update: A Report From the American Heart Association. Circulation. 2018;137(12):e67–e492. - PubMed
-
- Marelli AJ, Ionescu-Ittu R, Mackie AS, Guo L, Dendukuri N, Kaouache M. Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010. Circulation. 2014;130(9):749–756. - PubMed
-
- Schlichting LE, Insaf TZ, Zaidi AN, Lui GK, Van Zutphen AR. Maternal Comorbidities and Complications of Delivery in Pregnant Women With Congenital Heart Disease. J Am Coll Cardiol. 2019;73(17):2181–2191. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical