

Falls, healthcare resources and costs in older adults with insomnia treated with zolpidem, trazodone, or benzodiazepines
- PMID: 35658904
- PMCID: PMC9166444
- DOI: 10.1186/s12877-022-03165-6
Falls, healthcare resources and costs in older adults with insomnia treated with zolpidem, trazodone, or benzodiazepines
Abstract
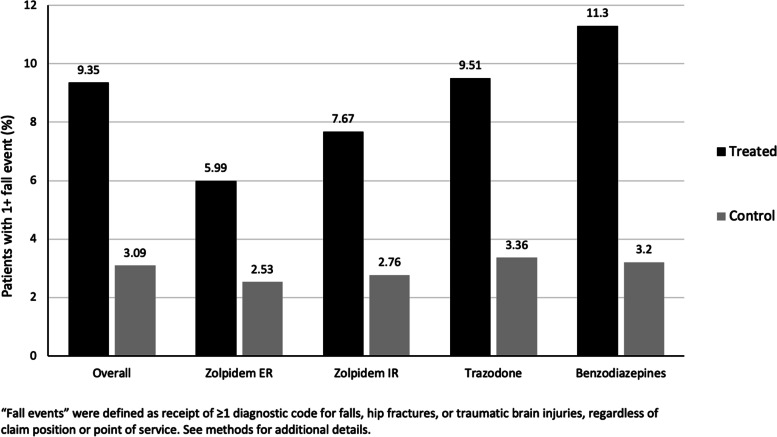
Background: Falls are the leading cause of injury-related death among older Americans. While some research has found that insomnia heightens falls, health care resource utilization (HCRU) and costs, the impact of insomnia treatments on fall risk, mortality, HCRU and costs in the elderly population, which could be of substantial interest to payers, has not been fully elucidated. This study evaluated the risk of falls and related consequences among adults ≥ 65 years of age treated with common prescription medications for insomnia compared with non-sleep disordered controls.
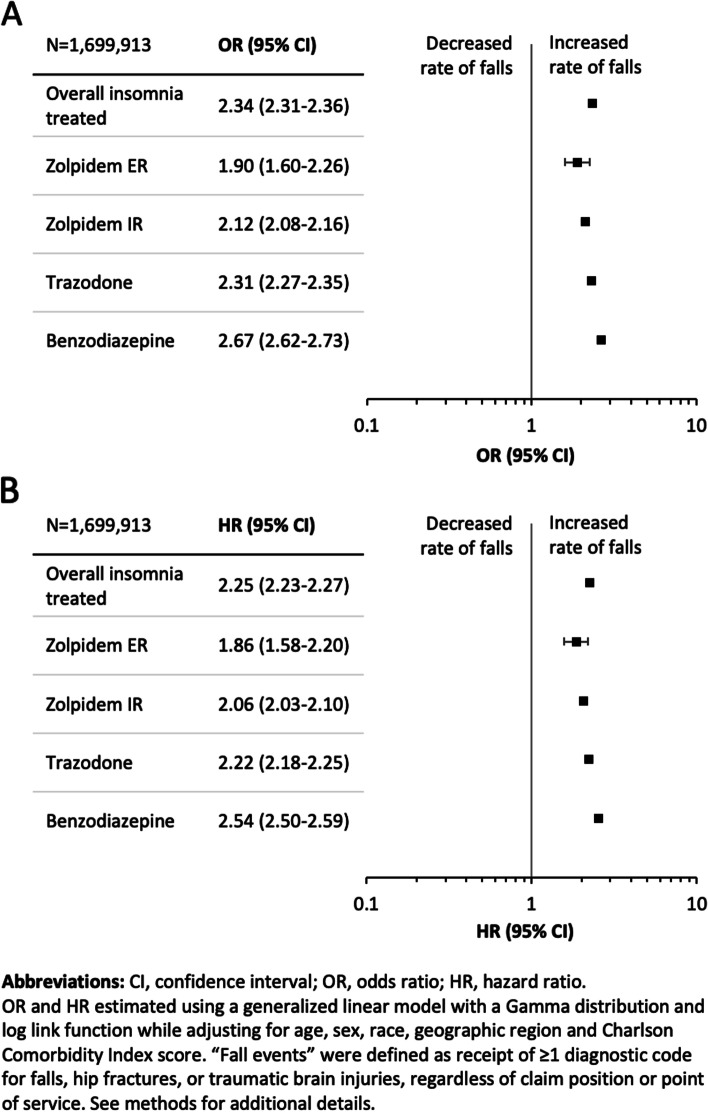
Methods: This was a retrospective cohort analysis of deidentified Medicare claims from January 2011 through December 2017. Medicare beneficiaries treated for insomnia receiving zolpidem extended-release, zolpidem immediate-release, trazodone, or benzodiazepines were matched with non-sleep disordered controls. The main outcomes were falls, mortality, healthcare resource utilization (HCRU), and medical costs during the 12 months following the earliest fill date for the insomnia medication of interest. Generalized linear models controlled for several key covariates, including age, race, sex, geographic region and Charlson Comorbidity Index score.
Results: The study included 1,699,913 Medicare beneficiaries (59.9% female, mean age 75 years). Relative to controls, adjusted analyses showed that beneficiaries receiving insomnia medication experienced over twice as many falls (odds ratio [OR] = 2.34, 95% CI: 2.31-2.36). In adjusted analyses, patients receiving benzodiazepines or trazodone had the greatest risk. Crude all-cause mortality rates were 15-times as high for the insomnia-treated as controls. Compared with controls, beneficiaries receiving insomnia treatment demonstrated higher estimated adjusted mean number of inpatient, outpatient, and emergency department visits and longer length of inpatient stay. All-cause total adjusted mean costs were higher among insomnia treated patients ($967 vs $454).
Conclusions: Individuals receiving insomnia treatment had an increased risk of falls and mortality and higher HCRU and costs compared with matched beneficiaries without sleep disorders. Trazodone and benzodiazepines were associated with the greatest risk of falls. This analysis suggests that significant risks are associated with common, older generation insomnia medication treatments in the elderly. Nonetheless, these results should be interpreted with caution as the use of these medications may be indicative of underlying morbidity with potential for residual confounding.
Keywords: Cost; Falls; Insomnia; Medicare; Older adults; Utilization.
© 2022. The Author(s).
Conflict of interest statement
EMW received compensation for consulting on this study. EMW's institution has received research funding from the AASM Foundation, US DoD, Merck, ResMed and ResMed Foundation. EMW has served as a scientific consultant to DayZz, Eisai, Merck, and Purdue, and is an equity shareholder in WellTap. TJ, FF and NA are employees of Eisai, Inc. DTA, WW and ZW are employees of Genesis Research, which received compensation for conducting this study.
Figures
References
-
- Croke L. Beers criteria for inappropriate medication use in older patients: an update from the AGS. Am Fam Physician. 2020;101(1):56–57. - PubMed
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5th. Arlington: American Psychiatric Publishing; 2013.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
