

Comparative analysis of background EEG activity based on MRI findings in neonatal hypoxic-ischemic encephalopathy: a standardized, low-resolution, brain electromagnetic tomography (sLORETA) study
- PMID: 35659637
- PMCID: PMC9164875
- DOI: 10.1186/s12883-022-02736-9
Comparative analysis of background EEG activity based on MRI findings in neonatal hypoxic-ischemic encephalopathy: a standardized, low-resolution, brain electromagnetic tomography (sLORETA) study
Abstract
Background: It is important to assess the degree of brain injury and predict long-term outcomes in neonates diagnosed with hypoxic-ischemic encephalopathy (HIE). However, routine studies, including magnetic resonance imaging (MRI) and conventional encephalography (EEG) or amplitude-integrated EEG (aEEG), have their own limitations in terms of availability and accuracy of evaluation. Recently, quantitative EEG (qEEG) has been shown to improve the predictive reliability of neonatal HIE and has been further refined with brain mapping techniques.
Methods: We investigated background EEG activities in 29 neonates with HIE who experienced therapeutic hypothermia, via qEEG using a distributed source model. MRI images were evaluated and classified into two groups (normal-to-mild injury vs moderate-to-severe injury), based on a scoring system. Non-parametric statistical analysis using standardized low-resolution brain electromagnetic tomography was performed to compare the current density distribution of four frequency bands (delta, theta, alpha, and beta) between the two groups.
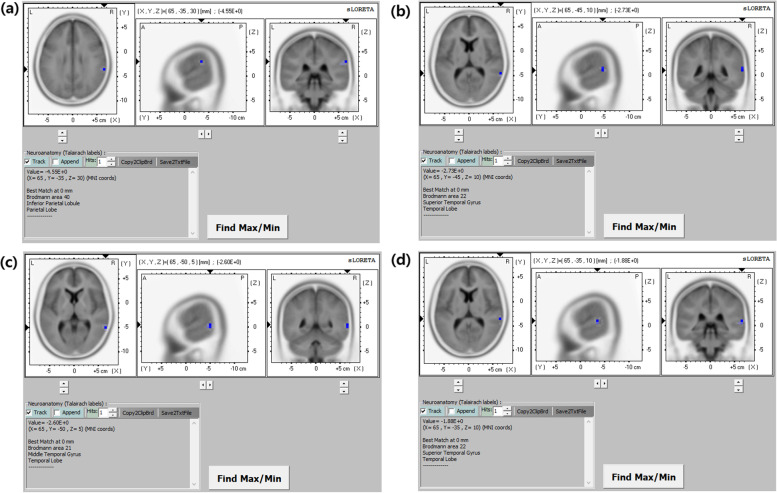
Results: Electrical neuronal activities were significantly lower in the moderate-to-severe injury group compared with the normal-to-mild injury group. Background EEG activities in moderate-to-severe HIE were most significantly reduced in the temporal and parietal lobes. Quantitative EEG also revealed a decrease in background activity at all frequency bands, with a maximum in decrease in the delta component. The maximum difference in current density was found in the inferior parietal lobule of the right parietal lobe for the delta frequency band.
Conclusions: Our study demonstrated quantitative and topographical changes in EEG in moderate-to-severe neonatal HIE. They also suggest possible implementation and evaluation of conventional EEG and aEEG in neonatal HIE. The findings have implications as biomarkers in the assessment of neonatal HIE.
Keywords: Distributed source model; Hypoxic-ischemic encephalopathy (HIE); Quantitative electroencephalography (qEEG); Standardized low-resolution brain electromagnetic tomography (sLORETA).
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Therapeutic hypothermia in neonatal hypoxic ischemic encephalopathy: electrographic seizures and magnetic resonance imaging evidence of injury.J Pediatr. 2013 Aug;163(2):465-70. doi: 10.1016/j.jpeds.2013.01.041. Epub 2013 Feb 26. J Pediatr. 2013. PMID: 23452588
-
Opioid analgesia and temperature regulation are associated with EEG background activity and MRI outcomes in neonates with mild-to-moderate hypoxic-ischemic encephalopathy undergoing therapeutic hypothermia.Eur J Paediatr Neurol. 2022 Jul;39:11-18. doi: 10.1016/j.ejpn.2022.04.001. Epub 2022 Apr 16. Eur J Paediatr Neurol. 2022. PMID: 35598572
-
Evaluation of Prognostic Findings in Newborns with Hypoxic Ischemic Encephalopathy: 5-Year Experience.Ther Hypothermia Temp Manag. 2025 Jun;15(2):97-103. doi: 10.1089/ther.2025.0011. Epub 2025 Mar 31. Ther Hypothermia Temp Manag. 2025. PMID: 40160108
-
Mild Hypoxic-Ischemic Encephalopathy: Can Neurophysiological Monitoring Predict Unfavorable Neurological Outcome? A Systematic Review and Meta-analysis.Am J Perinatol. 2023 Jun;40(8):833-838. doi: 10.1055/s-0041-1736593. Epub 2021 Oct 19. Am J Perinatol. 2023. PMID: 34666398
-
The Term Newborn: Evaluation for Hypoxic-Ischemic Encephalopathy.Clin Perinatol. 2021 Aug;48(3):681-695. doi: 10.1016/j.clp.2021.05.014. Clin Perinatol. 2021. PMID: 34353587 Review.
Cited by
-
High-beta oscillations at EEG resting state and hyperconnectivity of pain circuitry in fibromyalgia: an exploratory cross-sectional study.Front Neurosci. 2023 Nov 27;17:1233979. doi: 10.3389/fnins.2023.1233979. eCollection 2023. Front Neurosci. 2023. PMID: 38089976 Free PMC article.
-
Quantitative EEG and prediction of outcome in neonatal encephalopathy: a review.Pediatr Res. 2024 Jul;96(1):73-80. doi: 10.1038/s41390-024-03138-y. Epub 2024 Mar 19. Pediatr Res. 2024. PMID: 38503980 Review.
References
-
- Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, et al. Heart disease and stroke statistics 2009 update: a report from the American Heart Association statistics committee and stroke statistics subcommittee. Circulation. 2009;119:e21–181. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
