

The relative effects of non-pharmaceutical interventions on wave one Covid-19 mortality: natural experiment in 130 countries
- PMID: 35659646
- PMCID: PMC9165709
- DOI: 10.1186/s12889-022-13546-6
The relative effects of non-pharmaceutical interventions on wave one Covid-19 mortality: natural experiment in 130 countries
Abstract
Background: Non-pharmaceutical interventions have been implemented around the world to control Covid-19 transmission. Their general effect on reducing virus transmission is proven, but they can also be negative to mental health and economies, and transmission behaviours can also change voluntarily, without mandated interventions. Their relative impact on Covid-19 attributed mortality, enabling policy selection for maximal benefit with minimal disruption, is not well established due to a lack of definitive methods.
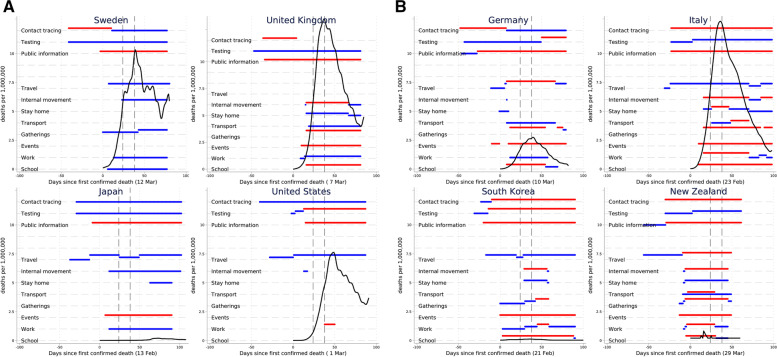
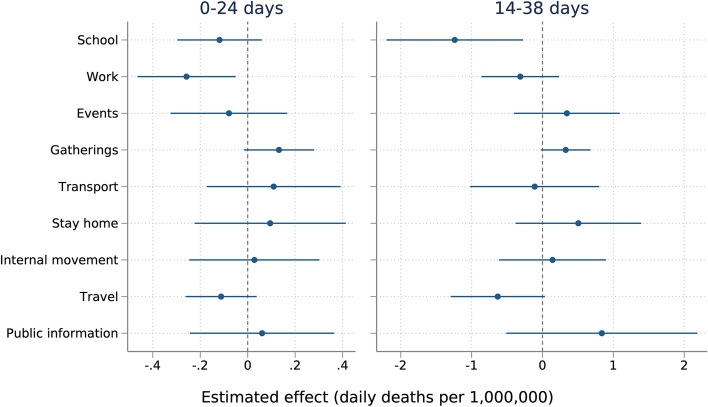
Methods: We examined variations in timing and strictness of nine non-pharmaceutical interventions implemented in 130 countries and recorded by the Oxford COVID-19 Government Response Tracker (OxCGRT): 1) School closing; 2) Workplace closing; 3) Cancelled public events; 4) Restrictions on gatherings; 5) Closing public transport; 6) Stay at home requirements ('Lockdown'); 7) Restrictions on internal movement; 8) International travel controls; 9) Public information campaigns. We used two time periods in the first wave of Covid-19, chosen to limit reverse causality, and fixed country policies to those implemented: i) prior to first Covid-19 death (when policymakers could not possibly be reacting to deaths in their own country); and, ii) 14-days-post first Covid-19 death (when deaths were still low, so reactive policymaking still likely to be minimal). We then examined associations with daily deaths per million in each subsequent 24-day period, which could only be affected by the intervention period, using linear and non-linear multivariable regression models. This method, therefore, exploited the known biological lag between virus transmission (which is what the policies can affect) and mortality for statistical inference.
Results: After adjusting, earlier and stricter school (- 1.23 daily deaths per million, 95% CI - 2.20 to - 0.27) and workplace closures (- 0.26, 95% CI - 0.46 to - 0.05) were associated with lower Covid-19 mortality rates. Other interventions were not significantly associated with differences in mortality rates across countries. Findings were robust across multiple statistical approaches.
Conclusions: Focusing on 'compulsory', particularly school closing, not 'voluntary' reduction of social interactions with mandated interventions appears to have been the most effective strategy to mitigate early, wave one, Covid-19 mortality. Within 'compulsory' settings, such as schools and workplaces, less damaging interventions than closing might also be considered in future waves/epidemics.
Keywords: Covid-19; Health policy; Public health.
© 2022. The Author(s).
Conflict of interest statement
JS is an Editorial Board member at BMC Health Services Research. All other authors declare that they have no competing interests.
Figures
References
-
- Hsiang S, Allen D, Annan-Phan S, Bell K, Bolliger I, Chong T, et al. The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature. 2020;584:262–7. https://www.nature.com/articles/s41586-020-2404-8. - PubMed
-
- Hale T, Webster S, Petherick A, Phillips T, Kira B. Oxford covid-19 government response tracker: Blavatnik School of Government. Oxford; 2020. p. 25. - PubMed
-
- Adams-Prassl A, Boneva T, Golin M, Rauh C. The impact of the coronavirus lockdown on mental health: evidence from the US. 2020.
-
- Fernandes N. Economic effects of coronavirus outbreak (COVID-19) on the world economy. 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
