

Association of Thromboxane Generation With Survival in Aspirin Users and Nonusers
- PMID: 35660296
- PMCID: PMC12175083
- DOI: 10.1016/j.jacc.2022.04.034
Association of Thromboxane Generation With Survival in Aspirin Users and Nonusers
Abstract
Background: Persistent systemic thromboxane generation, predominantly from nonplatelet sources, in aspirin (ASA) users with cardiovascular disease (CVD) is a mortality risk factor.
Objectives: This study sought to determine the mortality risk associated with systemic thromboxane generation in an unselected population irrespective of ASA use.
Methods: Stable thromboxane B2 metabolites (TXB2-M) were measured by enzyme-linked immunosorbent assay in banked urine from 3,044 participants (mean age 66 ± 9 years, 53.8% women) in the Framingham Heart Study. The association of TXB2-M to survival over a median observation period of 11.9 years (IQR: 10.6-12.7 years) was determined by multivariable modeling.
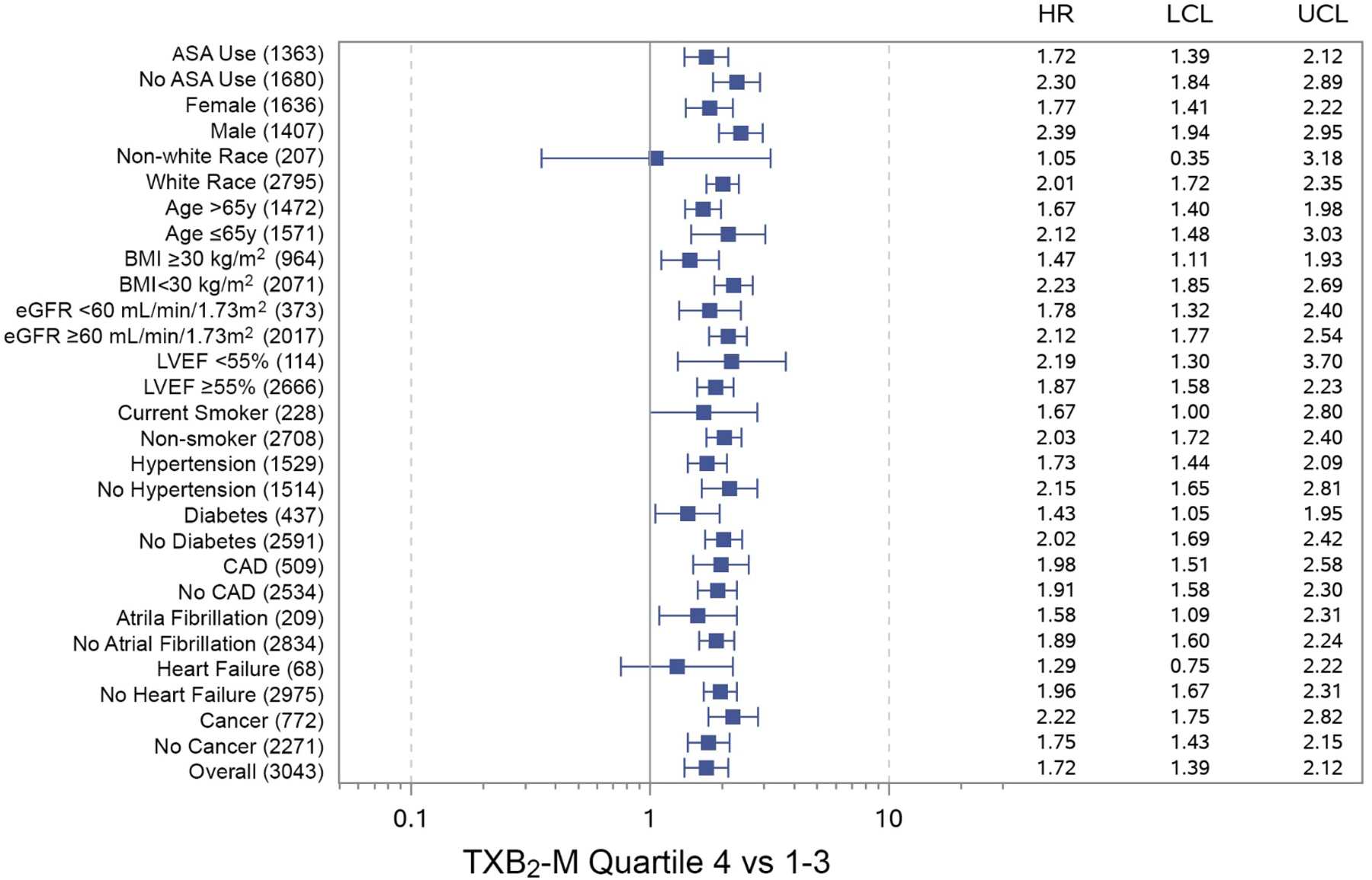
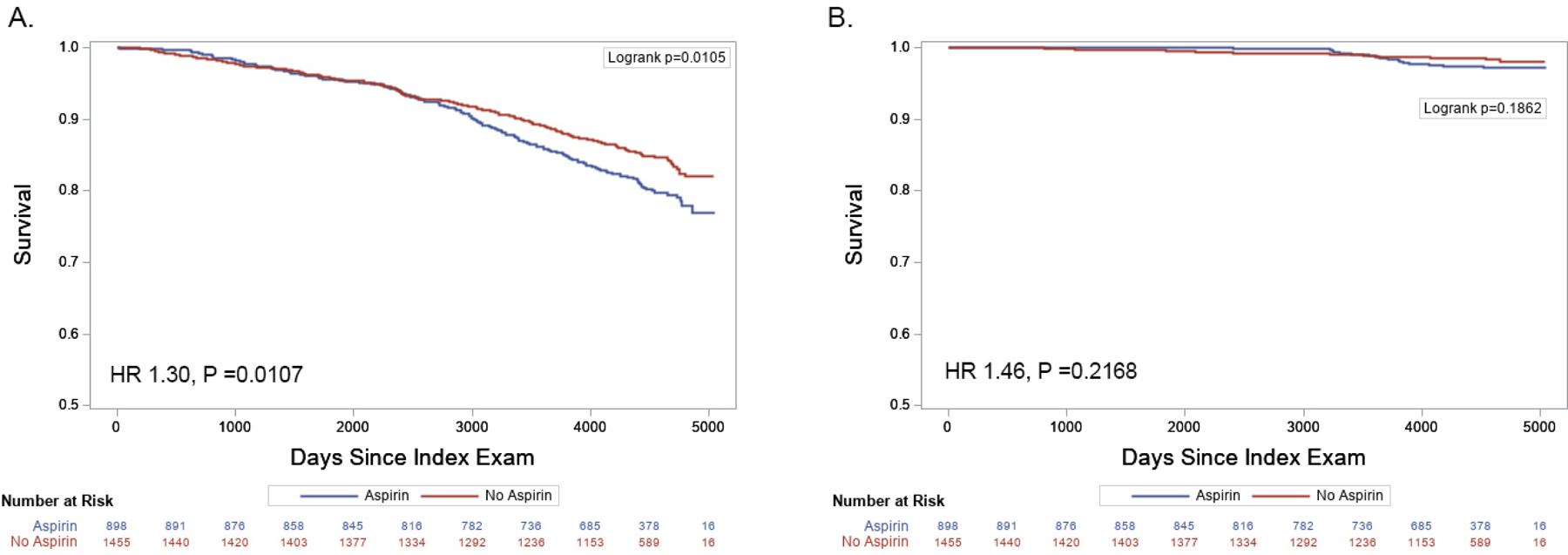
Results: In 1,363 (44.8%) participants taking ASA at the index examination, median TXB2-M were lower than in ASA nonusers (1,147 pg/mg creatinine vs 4,179 pg/mg creatinine; P < 0.0001). TXB2-M were significantly associated with all-cause and cardiovascular mortality irrespective of ASA use (HR: 1.96 and 2.41, respectively; P < 0.0001 for both) for TXB2-M in the highest quartile based on ASA use compared with lower quartiles, and remained significant after adjustment for mortality risk factors for similarly aged individuals (HR: 1.49 and 1.82, respectively; P ≤ 0.005 for both). In 2,353 participants without CVD, TXB2-M were associated with cardiovascular mortality in ASA nonusers (adjusted HR: 3.04; 95% CI: 1.29-7.16) but not in ASA users, while ASA use was associated with all-cause mortality in those with low (adjusted HR: 1.46; 95% CI: 1.14-1.87) but not elevated TXB2-M.
Conclusions: Systemic thromboxane generation is an independent risk factor for all-cause and cardiovascular mortality irrespective of ASA use, and its measurement may be useful for therapy modification, particularly in those without CVD.
Keywords: aspirin; isoprostane; mortality; platelets; thromboxane.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by a grant from American Heart Association (17GRNT3360007 to Dr Rade). The parent Framingham Heart Study was supported by contracts NO1-HC-25195, HHSN268201500001I, and 75N92019D00031 from the National Heart, Lung, and Blood Institute. Dr Vasan is supported in part by the Evans Medical Foundation and the Jay and Louis Coffman Endowment from the Department of Medicine, Boston University School of Medicine. The authors had sole control of the design of the study, collection, analyses, and dissemination of the data. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures






Comment in
-
Less Thromboxane, Longer Life.J Am Coll Cardiol. 2022 Jul 19;80(3):251-255. doi: 10.1016/j.jacc.2022.04.053. J Am Coll Cardiol. 2022. PMID: 35835497 No abstract available.
References
-
- Patrono C, Ciabattoni G, Davi G. Thromboxane biosynthesis in cardiovascular diseases. Stroke 1990;21:IV130–IV133. - PubMed
-
- Faraday N, Becker DM, Yanek LR et al. Relation between atherosclerosis risk factors and aspirin resistance in a primary prevention population. Am J Cardiol 2006;98:774–779. - PubMed
-
- Tantry US, Bliden KP, Gurbel PA. Overestimation of platelet aspirin resistance detection by thrombelastograph platelet mapping and validation by conventional aggregometry using arachidonic acid stimulation. J Am Coll Cardiol 2005;46:1705–1709. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
