

The host response in different aetiologies of community-acquired pneumonia
- PMID: 35660785
- PMCID: PMC9155985
- DOI: 10.1016/j.ebiom.2022.104082
The host response in different aetiologies of community-acquired pneumonia
Abstract
Background: Community-acquired pneumonia (CAP) can be caused by a variety of pathogens, of which Streptococcus pneumoniae, Influenza and currently SARS-CoV-2 are the most common. We sought to identify shared and pathogen-specific host response features by directly comparing different aetiologies of CAP.
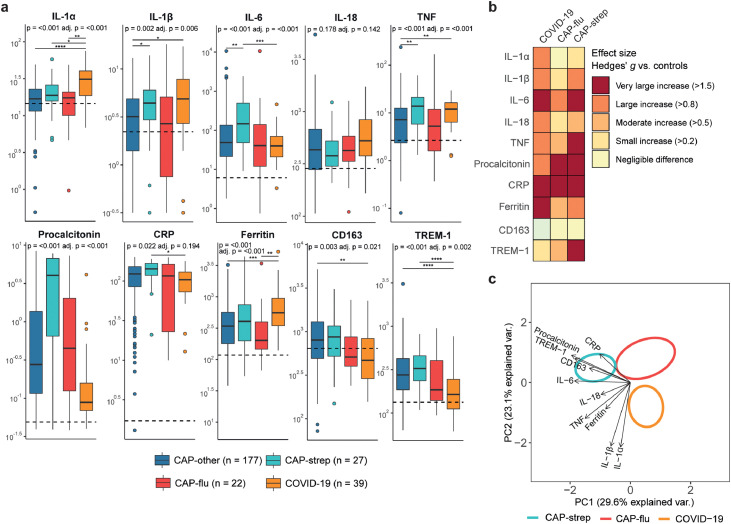
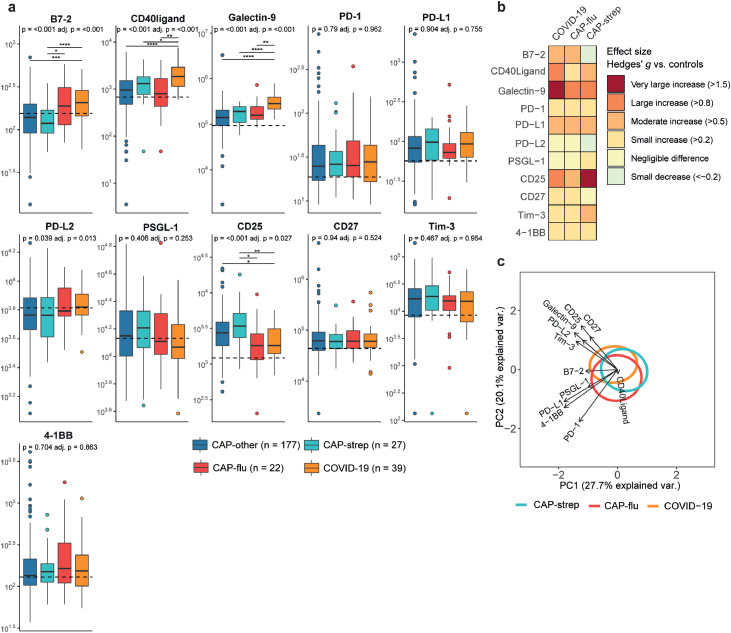
Methods: We measured 72 plasma biomarkers in a cohort of 265 patients hospitalized for CAP, all sampled within 48 hours of admission, and 28 age-and sex matched non-infectious controls. We stratified the biomarkers into several pathophysiological domains- antiviral response, vascular response and function, coagulation, systemic inflammation, and immune checkpoint markers. We directly compared CAP caused by SARS-CoV-2 (COVID-19, n=39), Streptococcus pneumoniae (CAP-strep, n=27), Influenza (CAP-flu, n=22) and other or unknown pathogens (CAP-other, n=177). We adjusted the comparisons for age, sex and disease severity scores.
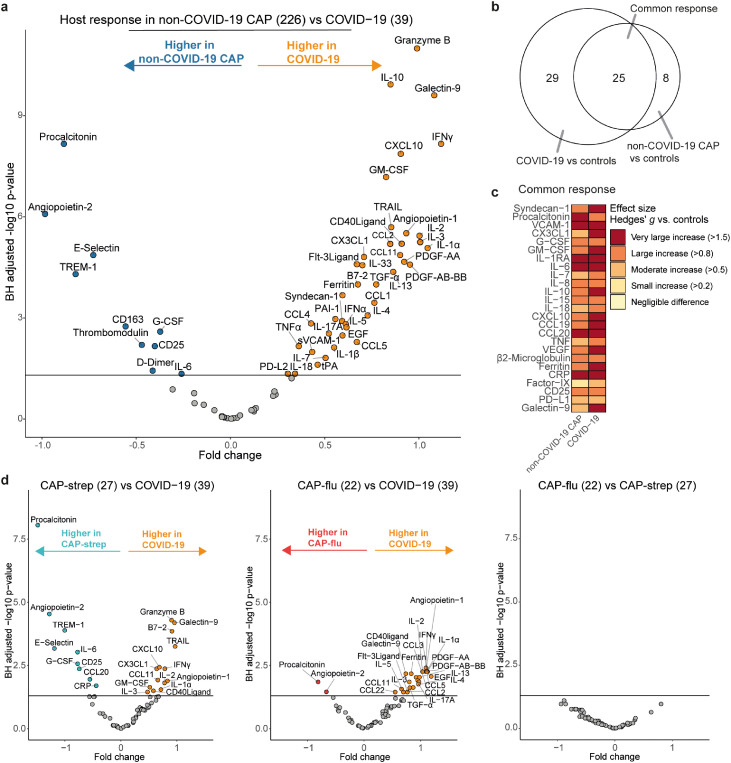
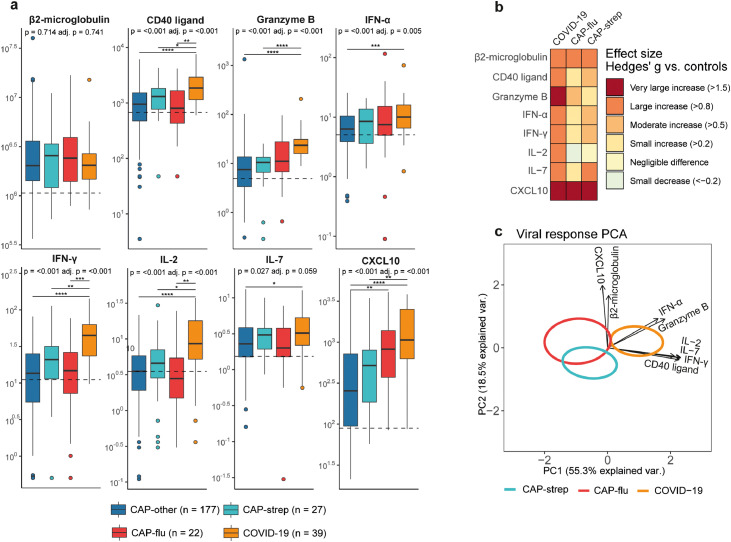
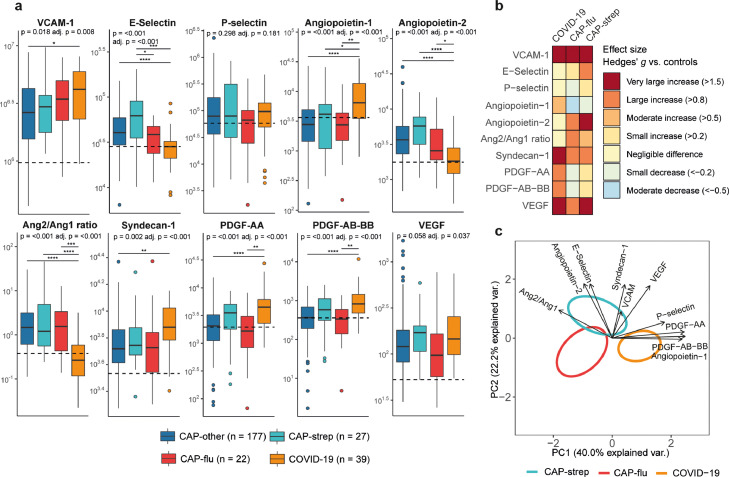
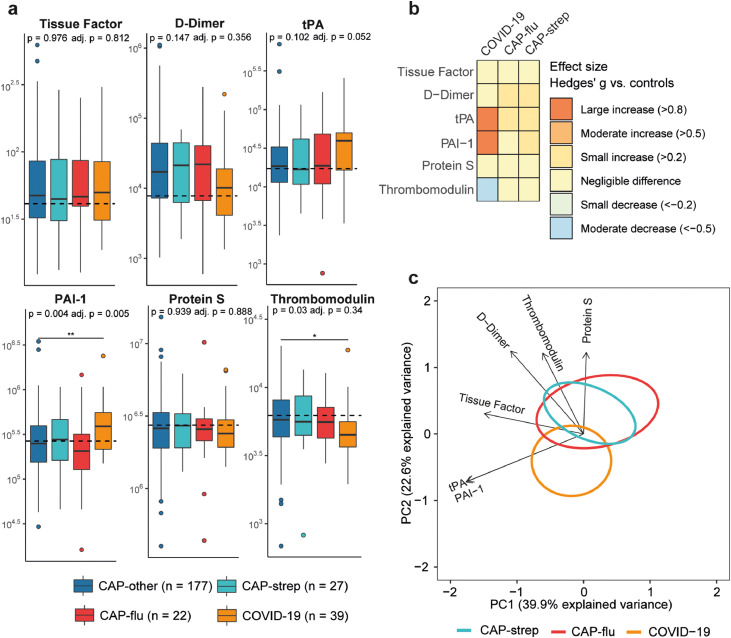
Findings: Biomarkers reflective of a stronger cell-mediated antiviral response clearly separated COVID-19 from other CAPs (most notably granzyme B). Biomarkers reflecting activation and function of the vasculature showed endothelial barrier integrity was least affected in COVID-19, while glycocalyx degradation and angiogenesis were enhanced relative to other CAPs. Notably, markers of coagulation activation, including D-dimer, were not different between the CAP groups. Ferritin was most increased in COVID-19, while other systemic inflammation biomarkers such as IL-6 and procalcitonin were highest in CAP-strep. Immune checkpoint markers showed distinctive patterns in viral and non-viral CAP, with highly elevated levels of Galectin-9 in COVID-19.
Interpretation: Our investigation provides insight into shared and distinct pathophysiological mechanisms in different aetiologies of CAP, which may help guide new pathogen-specific therapeutic strategies.
Funding: This study was financially supported by the Dutch Research Council, the European Commission and the Netherlands Organization for Health Research and Development.
Keywords: Aetiology; COVID-19; Community-acquired pneumonia; Host response; Influenza; Streptococcus pneumoniae.
Copyright © 2022 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests JS was on the Data Safety Monitoring Board of the Pointer trial (ISRCTN33682933), and is the Vice President of the European Society of Gastrointestinal and Abdominal Radiology. All other authors declare no conflict of interests.
Figures
References
-
- GBD 2016 Lower Respiratory Infections Collaborators Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018;18(11):1191–1210. - PMC - PubMed
-
- Torres A, Cilloniz C, Niederman MS, et al. Pneumonia. Nat Rev Dis Prim. 2021;7(1) - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
