

Teclistamab in Relapsed or Refractory Multiple Myeloma
- PMID: 35661166
- PMCID: PMC10587778
- DOI: 10.1056/NEJMoa2203478
Teclistamab in Relapsed or Refractory Multiple Myeloma
Abstract
Background: Teclistamab is a T-cell-redirecting bispecific antibody that targets both CD3 expressed on the surface of T cells and B-cell maturation antigen expressed on the surface of myeloma cells. In the phase 1 dose-defining portion of the study, teclistamab showed promising efficacy in patients with relapsed or refractory multiple myeloma.
Methods: In this phase 1-2 study, we enrolled patients who had relapsed or refractory myeloma after at least three therapy lines, including triple-class exposure to an immunomodulatory drug, a proteasome inhibitor, and an anti-CD38 antibody. Patients received a weekly subcutaneous injection of teclistamab (at a dose of 1.5 mg per kilogram of body weight) after receiving step-up doses of 0.06 mg and 0.3 mg per kilogram. The primary end point was the overall response (partial response or better).
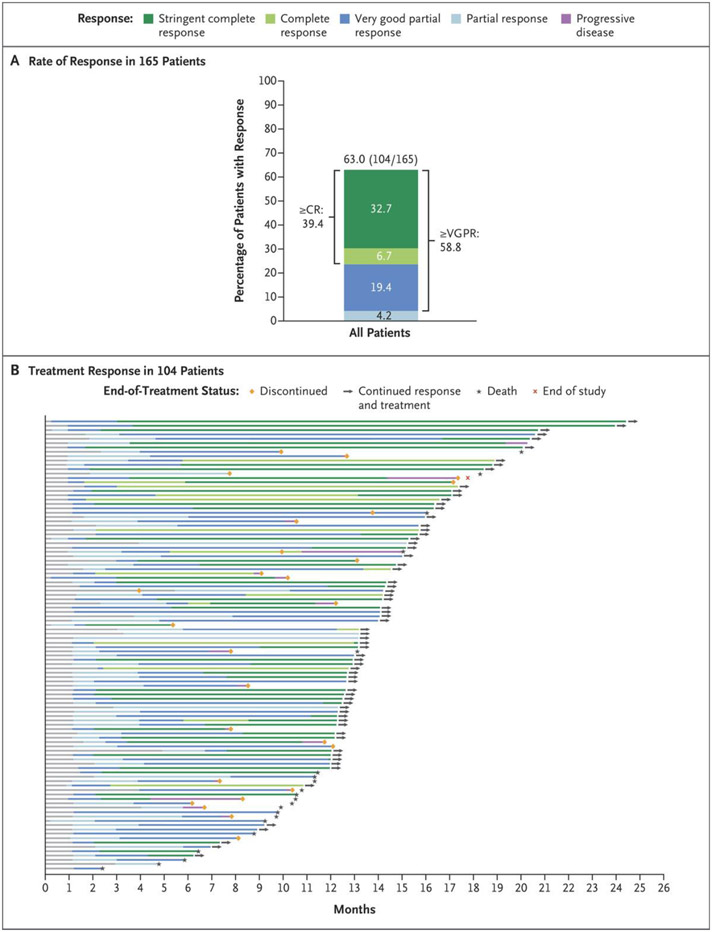
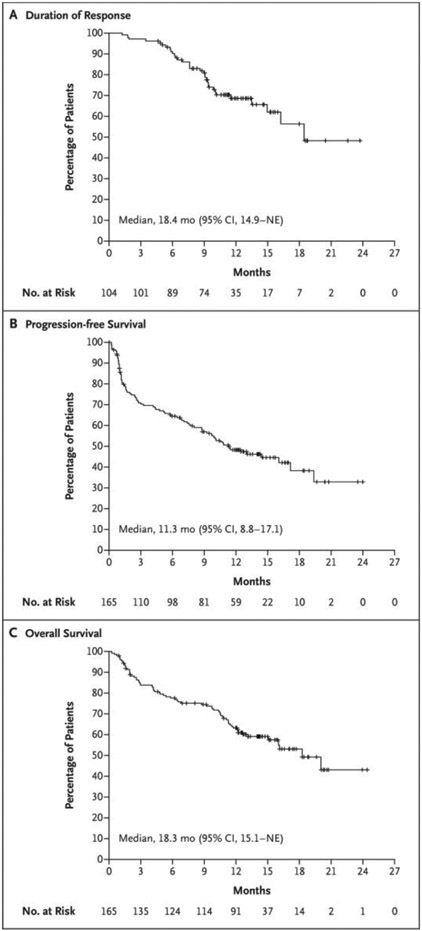
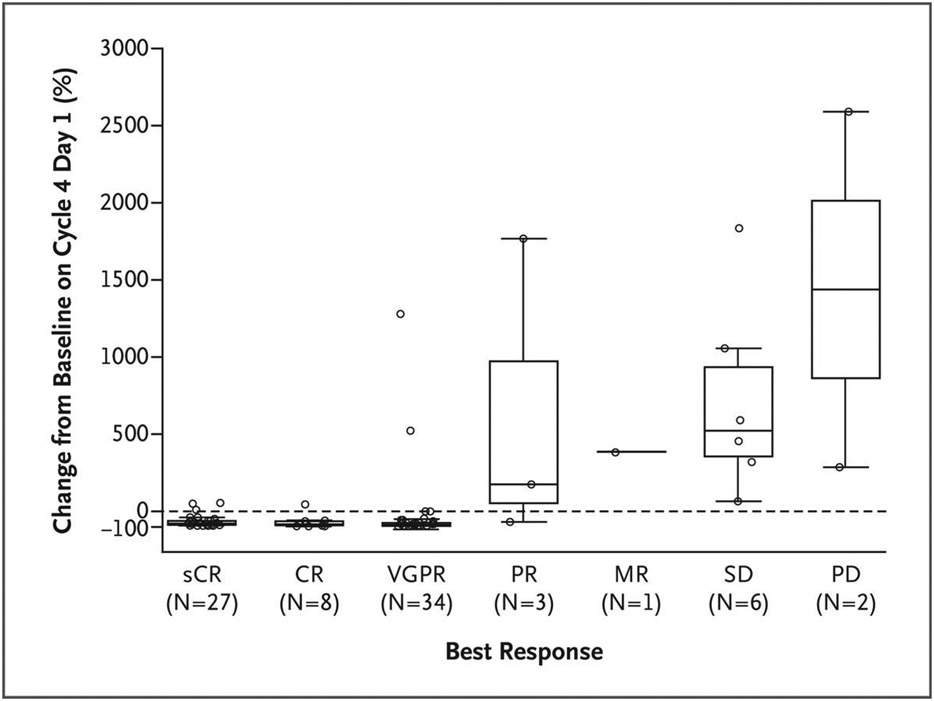
Results: Among 165 patients who received teclistamab, 77.6% had triple-class refractory disease (median, five previous therapy lines). With a median follow-up of 14.1 months, the overall response rate was 63.0%, with 65 patients (39.4%) having a complete response or better. A total of 44 patients (26.7%) were found to have no minimal residual disease (MRD); the MRD-negativity rate among the patients with a complete response or better was 46%. The median duration of response was 18.4 months (95% confidence interval [CI], 14.9 to not estimable). The median duration of progression-free survival was 11.3 months (95% CI, 8.8 to 17.1). Common adverse events included cytokine release syndrome (in 72.1% of the patients; grade 3, 0.6%; no grade 4), neutropenia (in 70.9%; grade 3 or 4, 64.2%), anemia (in 52.1%; grade 3 or 4, 37.0%), and thrombocytopenia (in 40.0%; grade 3 or 4, 21.2%). Infections were frequent (in 76.4%; grade 3 or 4, 44.8%). Neurotoxic events occurred in 24 patients (14.5%), including immune effector cell-associated neurotoxicity syndrome in 5 patients (3.0%; all grade 1 or 2).
Conclusions: Teclistamab resulted in a high rate of deep and durable response in patients with triple-class-exposed relapsed or refractory multiple myeloma. Cytopenias and infections were common; toxic effects that were consistent with T-cell redirection were mostly grade 1 or 2. (Funded by Janssen Research and Development; MajesTEC-1 ClinicalTrials.gov numbers, NCT03145181 and NCT04557098.).
Copyright © 2022 Massachusetts Medical Society.
Figures
Comment in
-
T-Cell Engagers - Modern Immune-Based Therapies for Multiple Myeloma.N Engl J Med. 2022 Aug 11;387(6):558-561. doi: 10.1056/NEJMe2209692. N Engl J Med. 2022. PMID: 35947712 No abstract available.
-
Teclistamab in Relapsed or Refractory Multiple Myeloma.N Engl J Med. 2022 Nov 3;387(18):1721. doi: 10.1056/NEJMc2211969. N Engl J Med. 2022. PMID: 36322859 No abstract available.
-
Teclistamab in Relapsed or Refractory Multiple Myeloma.N Engl J Med. 2022 Nov 3;387(18):1721-1722. doi: 10.1056/NEJMc2211969. N Engl J Med. 2022. PMID: 36322860 No abstract available.
References
-
- Kumar SK, Callander NS, Adekola K, et al. Multiple myeloma, version 3.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2020;18:1685–717. - PubMed
-
- Lonial S, Lee HC, Badros A, et al. Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2): a two-arm, randomised, open-label, phase 2 study. Lancet Oncol 2020;21:207–21. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials