

Six-Month Periodic Fasting in Patients With Type 2 Diabetes and Diabetic Nephropathy: A Proof-of-Concept Study
- PMID: 35661214
- PMCID: PMC9282263
- DOI: 10.1210/clinem/dgac197
Six-Month Periodic Fasting in Patients With Type 2 Diabetes and Diabetic Nephropathy: A Proof-of-Concept Study
Abstract
Context: Novel fasting interventions have gained scientific and public attention. Periodic fasting has emerged as a dietary modification promoting beneficial effects on metabolic syndrome.
Objective: Assess whether periodic fasting reduces albuminuria and activates nephropathy-driven pathways.
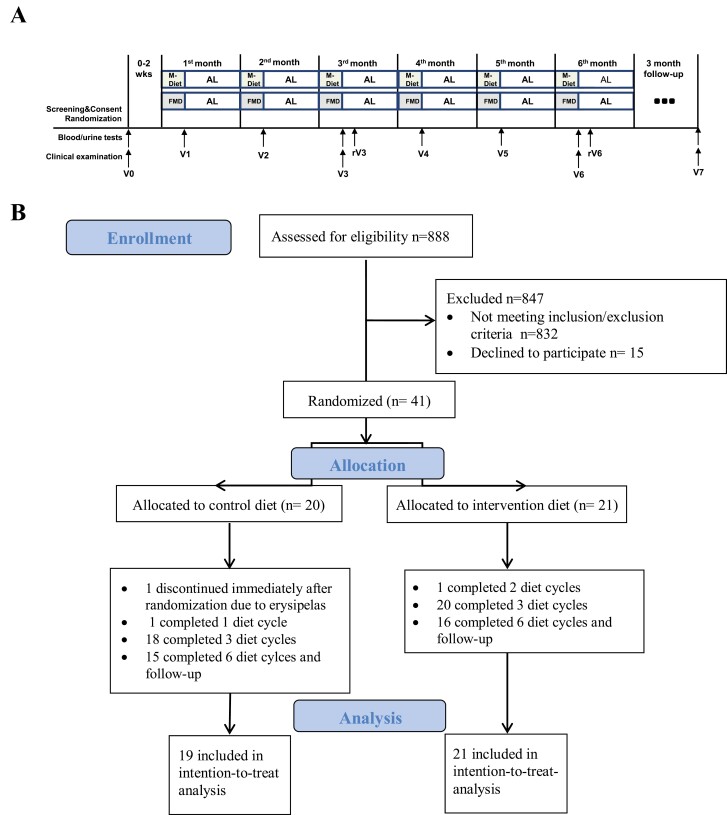
Design/participants: Proof-of-concept study where individuals with type 2 diabetes (n = 40) and increased albumin-to-creatinine ratio (ACR) were randomly assigned to receive a monthly fasting-mimicking diet (FMD) or a Mediterranean diet for 6 months with 3-month follow-up.
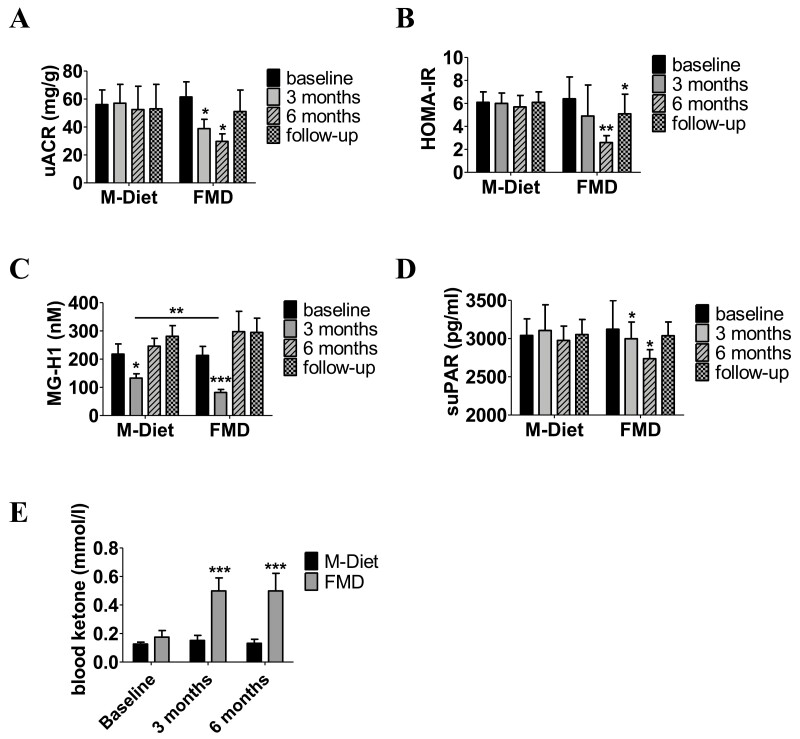
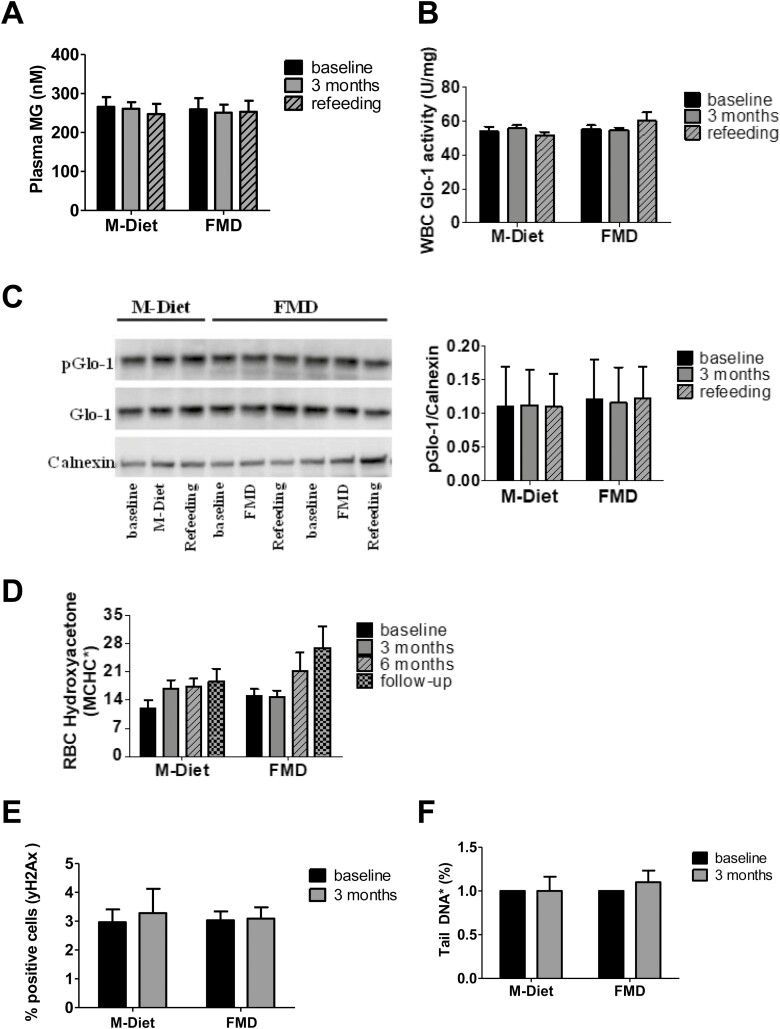
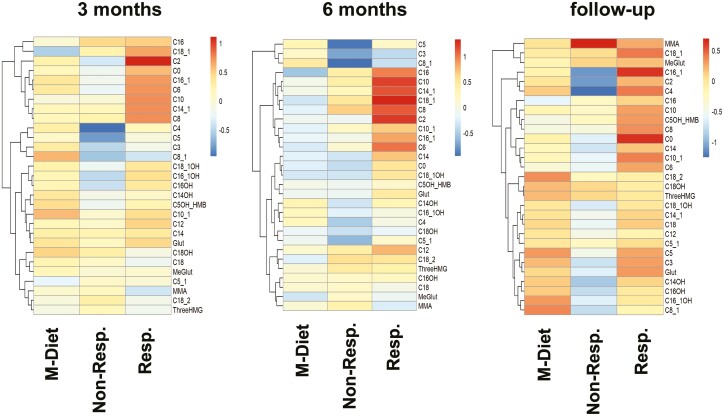
Main outcomes measures: Change in ACR was assessed by analysis of covariance adjusted for age, sex, weight loss, and baseline value. Prespecified subgroup analysis for patients with micro- vs macroalbuminuria at baseline was performed. Change in homeostatic model assessment for insulin resistance (HOMA-IR), circulating markers of dicarbonyl detoxification (methylglyoxal-derived hydroimidazolone 1, glyoxalase-1, and hydroxyacetone), DNA-damage/repair (phosphorylated histone H2AX), lipid oxidation (acylcarnitines), and senescence (soluble urokinase plasminogen activator receptor) were assessed as exploratory endpoints.
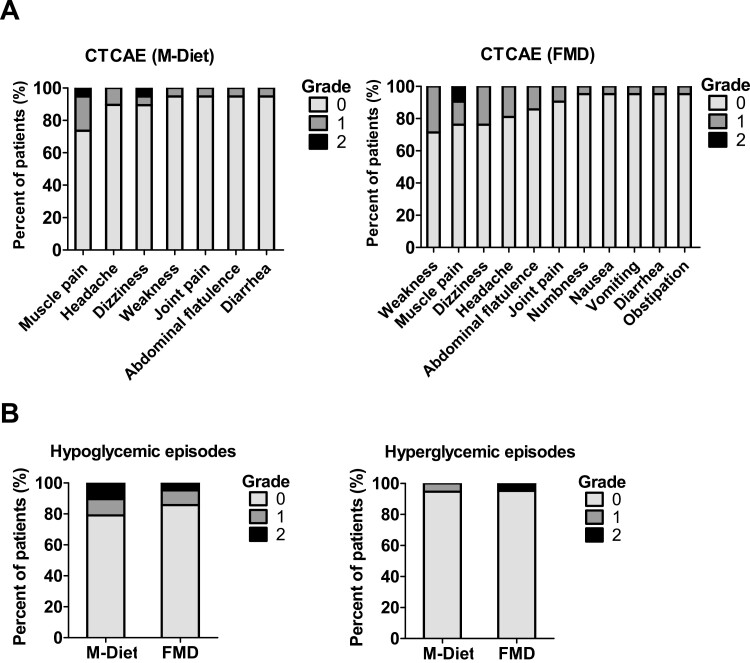
Results: FMD was well tolerated with 71% to 95% of the participants reporting no adverse effects. After 6 months, change in ACR was comparable between study groups [110.3 (99.2, 121.5) mg/g; P = 0.45]. FMD led to a reduction of ACR in patients with microalbuminuria levels at baseline [-30.3 (-35.7, -24.9) mg/g; P ≤ 0.05] but not in those with macroalbuminuria [434.0 (404.7, 463.4) mg/g; P = 0.23]. FMD reduced HOMA-IR [-3.8 (-5.6, -2.0); P ≤ 0.05] and soluble urokinase plasminogen activator receptor [-156.6 (-172.9, -140.4) pg/mL; P ≤ 0.05], while no change was observed in markers of dicarbonyl detoxification or DNA-damage/repair. Change in acylcarnitines was related to patient responsiveness to ACR improvement. At follow-up only HOMA-IR reduction [-1.9 (-3.7, -0.1), P ≤ 0.05]) was sustained.
Conclusions: Improvement of microalbuminuria and of markers of insulin resistance, lipid oxidation, and senescence suggest the potential beneficial effects of periodic fasting in type 2 diabetes.
Keywords: diabetic nephropathy; dicarbonyl detoxification; insulin resistance; lipid oxidation; periodic fasting; senescence.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Brenner B, Parving H-H, Mauer M, Ritz E. Diabetic nephropathy. In: Brenner BM, ed. Brenner and Rector’sThe Kidney, 8th ed. WB Saunders; 2006:1265-1298.
-
- Wanner C, Inzucchi SE, Lachin JM, et al. . Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323-334. - PubMed
-
- Ruggenenti P, Cravedi P, Remuzzi G. The RAAS in the pathogenesis and treatment of diabetic nephropathy. Nat Rev Nephrol. 2010;6(6):319-330. - PubMed
-
- Brownlee M. The pathobiology of diabetic complications: a unifying mechanism. Diabetes. 2005;54(6):1615-1625. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
