

Imaging in medically refractory epilepsy at 3 Tesla: a 13-year tertiary adult epilepsy center experience
- PMID: 35661273
- PMCID: PMC9167324
- DOI: 10.1186/s13244-022-01236-1
Imaging in medically refractory epilepsy at 3 Tesla: a 13-year tertiary adult epilepsy center experience
Abstract
Objectives: MRI negative epilepsy has evolved through increased usage of 3 T and insights from surgically correlated studies. The goal of this study is to describe dedicated 3 T epilepsy MRI findings in medically refractory epilepsy (MRE) patients at a tertiary epilepsy center to familiarize radiologists with an updated spectrum and frequency of potential imaging findings in the adult MRE population.
Methods: Included were all patients with MRE admitted to the epilepsy monitoring unit who were discussed at weekly interdisciplinary imaging conferences at Toronto Western Hospital with MRI studies (3 T with dedicated epilepsy protocol) performed between January 2008 and January 2021. Lesion characterization was performed by two readers based on most likely imaging diagnosis in consensus. Lobes involved per case were recorded.
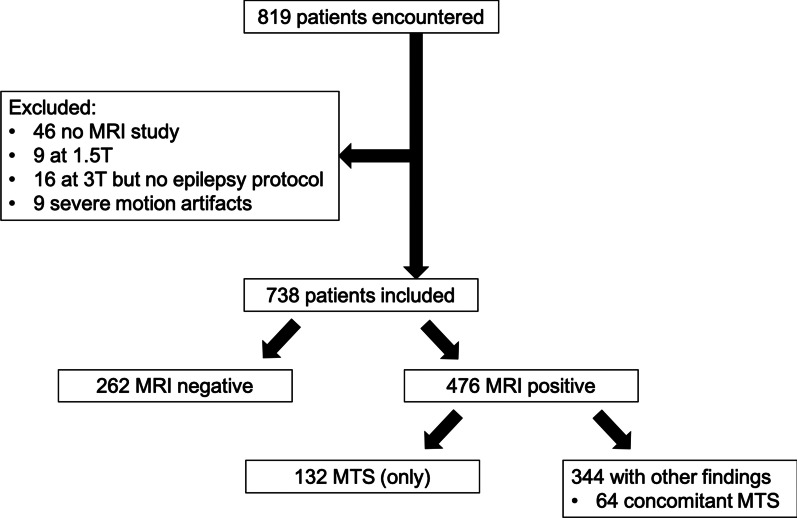
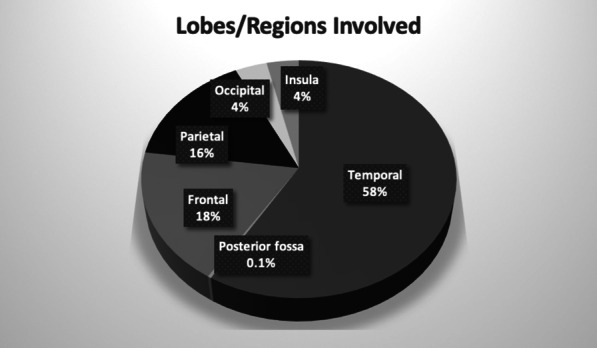
Results: A total of 738 patients (386 female; mean age 35 years, range 15-77) were included. A total of 262 patients (35.5%) were MRI negative. The most common imaging finding was mesial temporal sclerosis, seen in 132 patients (17.9%), followed by encephalomalacia and gliosis, either posttraumatic, postoperative, postischemic, or postinfectious in nature, in 79 patients (10.7%). The most common lobar involvement (either partially or uniquely) was temporal (341 cases, 58.6%). MRE patients not candidates for surgical resection were included in the study, as were newly described pathologies from surgically correlated studies revealing findings seen retrospectively on reported MRI negative exams (isolated enlargement of the amygdala, temporal pole white matter abnormality, temporal encephalocele).
Conclusion: This study provides an updated description of the spectrum of 3 T MRI findings in adult MRE patients from a tertiary epilepsy center.
Keywords: Drug resistant epilepsy; Epilepsy; Magnetic resonance imaging.
© 2022. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures
References
LinkOut - more resources
Full Text Sources
