

Choice of PD-L1 immunohistochemistry assay influences clinical eligibility for gastric cancer immunotherapy
- PMID: 35661944
- PMCID: PMC9226082
- DOI: 10.1007/s10120-022-01301-0
Choice of PD-L1 immunohistochemistry assay influences clinical eligibility for gastric cancer immunotherapy
Abstract
Background: Immune checkpoint inhibitors (ICI) are now standard-of-care treatment for patients with metastatic gastric cancer (GC). To guide patient selection for ICI therapy, programmed death ligand-1 (PD-L1) biomarker expression is routinely assessed via immunohistochemistry (IHC). However, with an increasing number of approved ICIs, each paired with a different PD-L1 antibody IHC assay used in their respective landmark trials, there is an unmet clinical and logistical need for harmonization. We investigated the interchangeability between the Dako 22C3, Dako 28-8 and Ventana SP-142 assays in GC PD-L1 IHC.
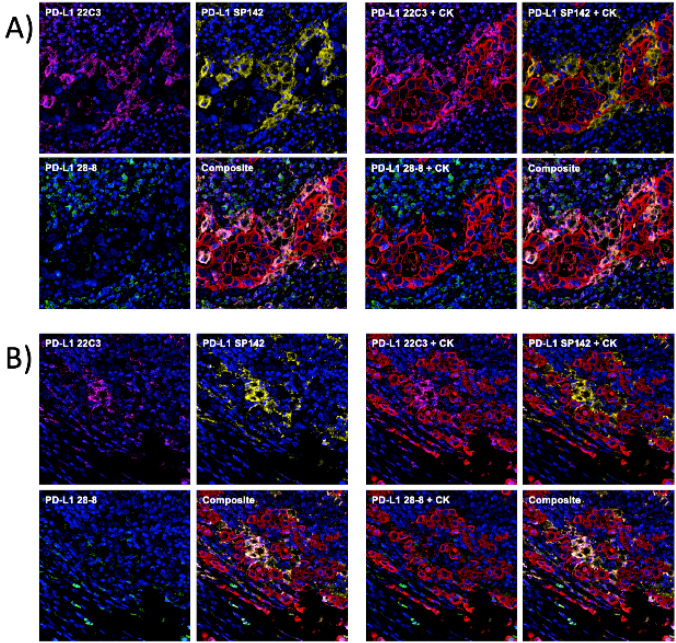
Methods: In this cross-sectional study, we scored 362 GC samples for PD-L1 combined positive score (CPS), tumor proportion score (TPS) and immune cells (IC) using a multiplex immunohistochemistry/immunofluorescence technique. Samples were obtained via biopsy or resection of gastric cancer.
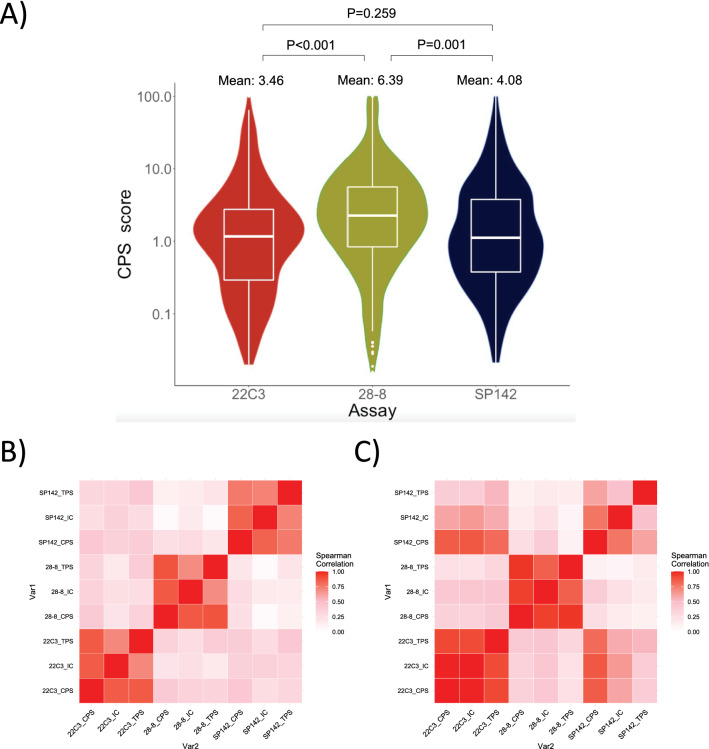
Results: The percentage of PD-L1-positive samples at clinically relevant CPS ≥ 1, ≥ 5 and ≥ 10 cut-offs for the 28-8 assay were approximately two-fold higher than that of the 22C3 (CPS ≥ 1: 70.3 vs 49.4%, p < 0.001; CPS ≥ 5: 29.1 vs 13.4%, p < 0.001; CPS ≥ 10: 13.7 vs 7.0%, p = 0.004). The mean CPS score on 28-8 assay was nearly double that of the 22C3 (6.39 ± 14.5 vs 3.46 ± 8.98, p < 0.001). At the clinically important CPS ≥ 5 cut-off, there was only moderate concordance between the 22C3 and 28-8 assays.
Conclusion: Our findings suggest that scoring PD-L1 CPS with the 28-8 assay may result in higher PD-L1 scores and higher proportion of PD-L1 positivity compared to 22C3 and other assays. Until stronger evidence of inter-assay concordance is found, we urge caution in treating the assays as equivalent.
Keywords: Biomarkers; Immune checkpoint inhibitors; Immunotherapy; Stomach neoplasms; Tumor.
© 2022. The Author(s).
Conflict of interest statement
RS has received honoraria from Bristol-Myers Squibb, Lilly, Roche, Taiho, Astra Zeneca, DKSH and MSD; has advisory activity with Bristol-Myers Squibb, Merck, Eisai, Bayer, Taiho, Novartis, MSD and AstraZeneca; received research funding from MSD and Paxman Coolers; and has received travel grants from AstraZeneca, Eisai, Roche and Taiho Pharmaceutical. WPY has advisory activity with Abbvie, Amgen, AstraZeneca, BMS, Ipsen, Novartis, MSD; is a speaker with Bayer, Eisai, Lilly, Sanofi, Taiho. The rest of the authors have no conflicts of interest to declare.
Figures
Comment in
-
Reply to: Letter to editor on the article "Choice of PD-L1 immunohistochemistry assay influences clinical eligibility for gastric cancer immunotherapy".Gastric Cancer. 2022 Nov;25(6):1133-1135. doi: 10.1007/s10120-022-01343-4. Epub 2022 Sep 24. Gastric Cancer. 2022. PMID: 36152122 No abstract available.
-
PD-L1 IHC testing: issues with interchangeability evidence based on laboratory-developed assays of unknown analytical performance.Gastric Cancer. 2022 Nov;25(6):1131-1132. doi: 10.1007/s10120-022-01336-3. Epub 2022 Sep 26. Gastric Cancer. 2022. PMID: 36163523 No abstract available.
References
-
- Shitara K, Ozguroglu M, Bang YJ, Di Bartolomeo M, Mandala M, Ryu MH, et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): a randomised, open-label, controlled, phase 3 trial. Lancet. 2018;392(10142):123–133. doi: 10.1016/S0140-6736(18)31257-1. - DOI - PubMed
-
- Fuchs CS, Doi T, Jang RW, Muro K, Satoh T, Machado M, et al. Safety and efficacy of pembrolizumab monotherapy in patients with previously treated advanced gastric and gastroesophageal junction cancer: phase 2 clinical KEYNOTE-059 trial. JAMA Oncol. 2018;4(5):e180013. doi: 10.1001/jamaoncol.2018.0013. - DOI - PMC - PubMed
-
- Shitara K, Van Cutsem E, Bang YJ, Fuchs C, Wyrwicz L, Lee KW, et al. Efficacy and safety of pembrolizumab or pembrolizumab plus chemotherapy vs chemotherapy alone for patients with first-line, advanced gastric cancer: the KEYNOTE-062 phase 3 randomized clinical trial. JAMA Oncol. 2020;6(10):1571–1580. doi: 10.1001/jamaoncol.2020.3370. - DOI - PMC - PubMed
-
- Sun JM, Shen L, Shah MA, Enzinger P, Adenis A, Doi T, et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet. 2021;398(10302):759–771. doi: 10.1016/S0140-6736(21)01234-4. - DOI - PubMed
-
- Drugs@FDA: FDA-approved drugs. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.... Accessed 4 Nov 2021
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
